

 What is lipedema (fat edema)?
What is lipedema (fat edema)?
In Hungary it is estimated that 5–8% of adult women may be affected, which corresponds to several hundred thousand individuals. Early recognition and multimodal treatment (compression, exercise, diet, pneumatic compression, and in some cases liposuction) can help alleviate symptoms and slow progression in the long term.
 Key point
Key point
Lipedema is a pathological adipose tissue disease, not simple obesity and not fluid retention (edema). Classic dieting alone does not reduce limb volume. The effective approach is a combination: compression garment + exercise + lifestyle changes + pneumatic compression + professional supervision.
Symptoms of lipedema and how to recognize it
Diagnosing lipedema does not require laboratory tests – the typical signs can be identified visually and by palpation. The four most important diagnostic criteria:
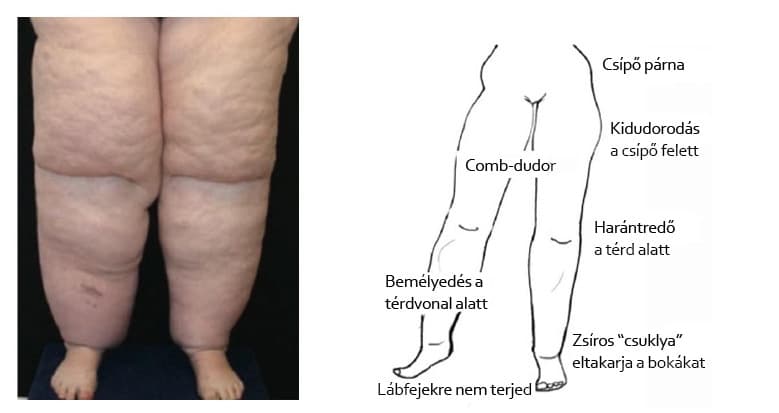
- Symmetric, bilateral fat accumulation on the hips, thighs, calves and often the upper arms, while the waist and abdominal area remain relatively slim.
- The foot and dorsum of the hand remain free – the fat mass stops in a "mansette-like" manner above the ankle and wrist. This is the clinical "mansette sign".
- Sensitive, easily bruising skin – small knocks or pressure can produce purple marks visible for weeks.
- Diet resistance – calorie deficit and dieting alone do not reduce the size of the affected regions, while non-lipedema areas (abdomen, breasts) lose volume.
Lipedema gradually worsens. The distinction between the four clinical stages is based not only on limb size but on skin surface appearance and tissue firmness:
| Stage | What do you see on the skin and tissue? | Direction of symptomatic treatment |
|---|---|---|
| 1. | Smooth skin surface, underlying soft, enlarged adipose tissue, tenderness and easy bruising tendency. | Compression garment + regular exercise. Pneumatic compression for daily maintenance use. |
| 2. | Uneven, "mattress-like" skin, small-to-medium palpable nodules in the adipose tissue. | Compression + physiotherapy + IPC combined, according to a protocol agreed with the treating physician. |
| 3. | Coarse skin waviness, large folds of adipose tissue, reduced mobility. | Complex decongestive therapy (CDT) + IPC; often under professional supervision. |
| 4. (lipo-lymphedema) | Secondary lymphedema accompanies lipedema; soft swelling appears on the foot as well. | CDT + IPC at low pressure + sometimes surgical consultation (liposuction, decompressive surgery). |
Lipedema or lymphedema? How do they differ?
Lipedema is most often confused with lymphedema because both cause swelling and a heavy-legged sensation. However, the two conditions arise from different mechanisms and require different treatment protocols – therefore accurate differentiation is the first step toward effective therapy.
| Feature | Lipedema | Lymphedema |
|---|---|---|
| What happens? | Pathological accumulation of subcutaneous adipose tissue | Disease of the lymphatic system, interstitial fluid stasis |
| Distribution | Symmetric, bilateral | Typically unilateral (except congenital primary forms) |
| Foot / dorsum of hand | Remains free – "mansette sign" | Usually involved, swollen |
| Skin | Sensitive, easily bruising | Firm, later stages become indurated |
| Stemmer sign | Negative (skin fold can be pinched up) | Positive (skin fold cannot be pinched up) |
| Effect of diet | Alone does not reduce limb size | Weight loss may alleviate but does not eliminate it |
| Sex distribution | Almost exclusively women | Both sexes (depending on indication) |
| Typical trigger event | Hormonal change (puberty, pregnancy, menopause) | Surgical procedure, radiotherapy, infection (secondary); congenital (primary) |
In advanced (stage 4) lipedema the two conditions can overlap: this is called lipo-lymphedema. In such cases both treatment logics are relevant, and clinicians typically prescribe an intensive version of complex decongestive therapy (CDT).
For a detailed clinical background on lymphedema, see the guide Lymphedema — forms, causes and stages.
Causes of lipedema
The exact trigger of lipedema is not fully clarified, but three main factor groups certainly play a role:
Genetic predisposition. The disease shows familial clustering: two-thirds of affected women report that their mother, sister or aunt had similar complaints. The exact inheritance pattern is under investigation, but a polygenic mechanism is likely — the combined effect of multiple genes increases susceptibility.
Hormonal factors. The disease almost always begins or worsens during hormonal life phases: puberty, start of hormonal contraception, pregnancy, postpartum period, or menopause. The presence of estrogen receptors in lipedematous adipose tissue may explain female predominance.
Microcirculatory and inflammatory factors. Lipedematous adipose tissue shows chronic, low-grade inflammation, capillary fragility and local hypoxia. Together these lead to pain sensation, edema tendency and sensitive skin.
It is important to know that lipedema is not a complication of overweight: it can appear in thin, normal-weight women. Obesity can worsen lipedema (and the two often coexist), but there is no causal relationship in the opposite direction.
Complications and long-term risks of lipedema
Untreated lipedema can lead to several complications:
- Lipo-lymphedema: in stages 3–4 the increased tissue mass can cause mechanical compression of lymphatic vessels, resulting in secondary lymphedema. The swelling then extends to the foot and becomes soft and indented (Stemmer sign may become positive).
- Venous insufficiency: increased tissue mass and reduced mobility can cause venous stasis, leading to spider veins and varicose veins and, in the long term, chronic venous insufficiency.
- Joint overload: prolonged mechanical load on the knee and hip can lead to early cartilage wear and gonarthrosis, especially in stage 3.
- Psychological burden: visible body-image change, chronic pain and often being misdiagnosed as obese can lead to depression, anxiety and eating disorders.
- Skin problems: between large fat folds intertrigo (skin inflammation), fungal infections and in advanced cases chronic wounds may develop.
These complications are not inevitable — early recognition and multimodal treatment (compression + exercise + lifestyle + IPC + specialist consultation) can effectively reduce their risk.
Pathological condition, not "simple" obesity!
Lipedema is one of the most frequently misdiagnosed women’s conditions: affected individuals typically visit multiple doctors for 10–15 years before receiving the correct diagnosis. During this time they are often told: “lose weight”, “exercise more”, “train yourself” — while classic calorie-restriction diets DO NOT reduce lipedematous areas.
Lipedematous adipose tissue is biologically different from the adipose tissue of metabolic obesity. The differences below can help with differentiation:
| Feature | Lipedema | Classic obesity |
|---|---|---|
| Distribution | Symmetric, lower body (hips, thighs, calves) | Generalized, includes abdominal and visceral regions |
| Effect of diet | Does not reduce affected regions | All regions decrease proportionally |
| Pain, tenderness | Typically present | Rare |
| Tendency to bruise | Typically present | Generally not |
| Onset linked to hormonal event | Yes (puberty, pregnancy, menopause) | Not necessarily |
If most of the above points fit you, it is worth consulting a lipedema-experienced specialist (lymphologist, vascular surgeon, or plastic surgeon with lipedema practice). Early diagnosis is decisive for long-term quality of life and progression.
Principles of home treatment for lipedema
Treatment of lipedema is multimodal: there is no single method that alone solves the problem. The most effective approach is based on four elements that should be applied in parallel.
1. Daily wear of a compression garment. Individually sized compression stockings or bib compression leggings of class II or III, worn from waking to bedtime. This is the foundation of treatment — other methods supplement its effectiveness.
2. Pneumatic compression (IPC). A home lymphatic massage device with 30–60 minutes of daily sessions at 30–60 mmHg. The device sequentially inflates the cuff air chambers and "smooths" fluid and venous blood along the limb. This is one of the most effective home maintenance tools.
3. Regular exercise. Swimming, water aerobics, walking, cycling while wearing compression. Physical activity improves venous return, reduces inflammation and can slow progression.
4. Anti-inflammatory lifestyle. Mediterranean-type diet, low carbohydrate intake, adequate hydration, sleep management, stress control.
The detailed selection logic for pneumatic compression devices is available on the Lipedema — fat edema category page, and the multi-indication hub can be found in the /compression-therapy-unit section. For differences between manual and machine lymphatic drainage see the Lymphatic drainage guide.
 Evidence for pneumatic compression in lipedema
Evidence for pneumatic compression in lipedema
Clinical studies on home pneumatic compression (IPC) in lipedema patients have expanded significantly in recent years. The following four randomized trials examined how limb volume, pain, fluid distribution and quality of life change with pneumatic treatment.
Atan and Bahar-Özdemir (2021) – RCT, 33 women, severe lipedema
In the study the combination of complete decongestive therapy (CDT) + exercise produced the largest reductions in limb volume, pain and physical function. IPC + exercise also produced significantly better results than exercise alone. Pneumatic compression is therefore a valuable component of the treatment package, especially in stages 1–2.1
Wright et al. (2023) – PCD + conservative care RCT
Pneumatic compression device + conservative care (PCD+CC) led to greater improvements in leg circumference, bioimpedance and pain scores than conservative care (compression garment + lifestyle) alone. SF-36 quality-of-life scores were also better in the PCD group.2
Herbst et al. (2025) – APCD lipedema RCT, 46 women
Thirty days of home APCD use (advanced pneumatic compression device) significantly reduced leg volume, extracellular and intracellular fluid, and subcutaneous adipose tissue thickness as confirmed by ultrasound. Quality of life (RAND SF-36) improved in 87.5% of the women studied.3
Esmer and Schingale (2024) – CDT + IPC slows progression
After one month of CDT + IPC in 22 women with lipedema, both intracellular and extracellular fluid volumes decreased. The authors suggest combined therapy may slow disease progression, which may be particularly important in stages 1–2.4
The consistent message of these four trials: pneumatic compression is not a magic cure by itself, but together with compression garments, exercise, physiotherapy and lifestyle changes it is a valuable, home-usable adjunct. The combined approach is the most effective.
Lipedema diet — what to eat and what to avoid?
The lipedema diet is not a classic weight-loss diet — the goal is to reduce inflammation and stabilize fluid balance rather than primarily restrict calories. Three approaches have become common in clinical practice:
Mediterranean-style diet. Plenty of vegetables, fruit, fish, olive oil, nuts, legumes. Moderate whole grains, little red meat, minimal refined sugar. Strong anti-inflammatory profile and sustainable long-term.
Low-carbohydrate intake (low-carb). Minimizing or excluding refined carbohydrates and gluten-containing grains. Many patients report significant reductions in pain and tenderness with lower carbohydrate intake.
Ketogenic diet. A strict variant where carbohydrate intake is kept below 20–50 grams per day. Clinical studies (RAD diet, ketogenic diet for lipedema) are promising, but long-term adherence is challenging. Recommended only under dietitian supervision.
To create an individualized plan, consult a dietitian experienced in lipedema. A detailed lipedema diet guide — meal plans, recipes, clinical evidence — will be presented in a separate article.
Physiotherapy for lipedema
The key criterion for exercise therapy in lipedema: exercise in compression garments. The compression garment supports lipedematous tissues, reduces joint load and optimizes venous return.
Recommended activities:
- Swimming and water aerobics: hydrostatic pressure provides natural compression and buoyancy reduces joint load. Practicing 2–3 times per week is especially recommended.
- Walking: 30 minutes daily in compression stockings. The calf muscle pump improves venous return.
- Cycling (indoor or outdoor): low-impact with good cardiovascular benefit.
- Functional strengthening exercises: using moderate weights with controlled range. Aim to maintain muscle mass, which improves metabolism.
Avoid HIIT (high-intensity interval training) and running on hard surfaces without compression — these may worsen symptoms. A detailed home protocol is provided in the lipedema physiotherapy article.
Surgical treatment of lipedema
For stage 3–4 lipedema, where conservative therapy no longer yields adequate results, surgical intervention may be considered. The most widespread methods are water-assisted liposuction (WAL) or tumescent liposuction — these differ from traditional suction lipectomy in that the lipedematous tissue is removed more gently, aiming to preserve lymphatic vessels.
Liposuction in lipedema is NOT a cosmetic procedure but a therapeutic surgery: its goals are to reduce tissue volume, relieve pain and restore mobility. Clinical studies with long-term (5–10 year) follow-up show favorable outcomes.
It is important to know that surgery does not replace conservative treatment — postoperatively you must continue compression, exercise, diet and pneumatic compression routines. Surgery can shift the stage forward, but it does not eliminate the disease’s nature.
The procedure is available both in Hungary and abroad. The key to selection is a plastic or vascular surgeon with lipedema-specific experience who has performed at least 50–100 similar operations.
Lifestyle advice and psychological support
Lipedema is a chronic disease that affects all aspects of quality of life. Alongside multimodal treatment, lifestyle elements and psychological support are as important as physical methods.
Hydration and metabolism. 2–2.5 liters of water daily to stabilize fluid balance. Reducing sodium intake lowers fluid retention.
Sleep and recovery. 7–8 hours of quality sleep per night. Sleep deprivation increases chronic inflammatory markers, which is particularly counterproductive in lipedema.
Stress management. Chronic stress raises cortisol levels, which promotes local inflammation. Meditation, yoga, breathing techniques and forest walks have all been shown to reduce cortisol.
Psychological support. Common comorbidities in women with lipedema include depression, anxiety, eating disorders and body-image disturbances. Affected individuals should consider consulting a psychologist, therapist or joining a lipedema support group. Understanding the nature of the disease — "it’s not your fault, this is a medical condition" — often brings significant relief.
In Hungary several lipedema patient organizations and online communities operate. These are important forums for sharing experiences, learning about new treatment options and receiving psychological support.
Deeper guides for lipedema management
Specific subtopics of lipedema are expanded in separate articles so that stage-level, dietary and physiotherapy recommendations receive sufficient depth. These will be available soon:
- Lipedema stages (1–4) — visual differentiation and stage-level management (coming soon)
- Lipedema vs. lymphedema — how to differentiate?
- Lipedema diet — anti-inflammatory approach and practical meal plans (coming soon)
- Lipedema physiotherapy — daily 15–30 minute home protocol (coming soon)
Currently available guides in the cluster:
- Lipedema — fat edema category — stage-level product recommendations and clinical evidence
- Lymphatic massage devices — multi-indication hub — pneumatic compression for all indications
- Lymphatic massage devices — purpose and how to choose? — technical selection guide
- Lymphatic drainage — manual and machine lymphatic massage — differences between the two methods
 Before you start home compression treatment
Before you start home compression treatment
Pneumatic compression is a safe procedure, but there are some conditions when consultation with a physician is required before use. Individual assessment is also warranted for compression garments.
When should you be cautious?
- Acute deep vein thrombosis or suspicion of it – treatment only with medical approval and monitoring.
- Severe heart failure – increased venous return may cause decompensation.
- Active skin infection or open wound in the treated area – not recommended until the infection heals.
- Severe peripheral arterial disease – individual assessment and low pressure are indicated.
- Untreated high blood pressure – stabilize first, then use on medical advice.
- Active malignant tumor in the treated region – only with oncologist approval.
 Important note
Important note
Pneumatic compression and compression garments are elements of complex lipedema care and do not replace medical or physiotherapy treatment. Always consult your treating physician before starting a new therapy, and begin initial sessions at low pressure and short duration.
Frequently asked questions
Lipedema is characterized by symmetric, disproportionate fat accumulation on the hips, thighs, calves and upper arms while the waist, foot and dorsum of the hand remain relatively slim. The skin is tender and easily bruises, and dieting alone does not reduce limb size. These signs should be evaluated by a specialist (lymphologist, vascular surgeon). The detailed differential table is in the above “Lipedema or lymphedema?” section.
In clinical practice the anti-inflammatory approach (Mediterranean diet, low carbohydrate intake, possibly ketogenic orientation) is common. Classic calorie-restriction dieting alone does not reduce lipedematous adipose tissue. A detailed dietary guide is covered in the lipedema diet article — meanwhile, consult a dietitian for an individualized plan.
In stages 1–2 a 4-chamber home device is generally sufficient (e.g. Power Q-2200, 1000 Plus, 1000 Premium) at 30–60 mmHg, starting from a lower level. In stage 3 a 6-chamber Power Q-8060 or the 12-chamber Power Q-8120 with finer sequential action may be advantageous. Detailed selection logic is on the Lipedema — fat edema category.
Lipedema is currently a chronic disease without a therapy that eliminates the cause. Multimodal treatment (compression, exercise, diet, pneumatic compression, and sometimes liposuction) can alleviate symptoms long term, slow progression and significantly improve quality of life. Early recognition and consistent treatment are key.
Water-assisted or tumescent liposuction can move the disease back by one stage (for example from stage 3 to 1–2) and significantly reduce pain, tissue volume and mobility limitations. However, it does not cure the disease — conservative treatment (compression, exercise, diet) must be continued after surgery. Clinical results over 5–10 years are favorable if the patient adheres to the postoperative routine.
The pool of lipedema specialists in Hungary is still small but growing. A lymphologist, vascular surgeon or plastic surgeon with a lipedema practice can establish the diagnosis and develop the treatment plan. Several lipedema patient organizations (Hungarian Lipedema Association, Facebook groups) help identify available specialists. Members often share names of physicians they have had positive experiences with.
 Summary — the key to successful lipedema management
Summary — the key to successful lipedema management
Sources
- Atan T, Bahar-Özdemir Y (2021). The Effects of Complete Decongestive Therapy or Intermittent Pneumatic Compression Therapy or Exercise Only in the Treatment of Severe Lipedema: A Randomized Controlled Trial. Lymphatic Research and Biology. DOI: 10.1089/lrb.2020.0019
- Wright T, Scarfino CD, O'Malley EM (2023). Effect of pneumatic compression device and stocking use on symptoms and quality of life in women with lipedema: A proof-in-principle randomized trial. Phlebology. DOI: 10.1177/02683555221145779
- Herbst KL, Zelaya C, Sommerville M, Zimmerman T, McHutchison L (2025). An Advanced Pneumatic Compression Therapy System Improves Leg Volume and Fluid, Adipose Tissue Thickness, Symptoms, and Quality of Life and Reduces Risk of Lymphedema in Women with Lipedema. Life (Basel). DOI: 10.3390/life15050725
- Esmer M, Schingale FJ (2024). Can Physical Therapy Techniques Slow Down the Progression of Lipedema?. Lymphatic Research and Biology. DOI: 10.1089/lrb.2024.0065
