Blog

The word “biohacking” has become a frequently used concept in the last decade: smart, targeted “tuning” of your own body with minimal time and money investment. With work, family and everyday life, often only a few hours per week remain for exercise, while maintaining muscle strength, endurance and body shape would require much more activity. Increasingly, people turn to muscle stimulators (EMS): a longer workout can be supplemented or partly replaced with 20–30 minutes per day.
There is a gap between “I can move it a little” and “I use it fully.” Load bridges that gap. Rehabilitation is not about rest but about gradually, intelligently dosed loading — that is what restores tissue, muscle and the nervous system to normal function.
The most common mistake is one of two extremes: either you are overly cautious and essentially “exercise” for months without meaningful load (and no real improvement occurs), or you try to progress too fast and overload. In this article I show the logical sequence of loading, how to progress safely, and where each tool helps.
“Go to physiotherapy.” – that’s what you hear in the clinic, and you nod while having no idea who to turn to. A physiotherapist? A physio (physiotherapy practitioner)? Are they the same? And where does the masseur fit in, and that so‑called “medical fitness” trainer your neighbour mentioned? Rehabilitation is team work, but if you don’t know who does what, you can easily knock on the wrong door — and lose valuable weeks.

I receive letters every day from people who have been carrying some complaint for weeks, months, sometimes years. Everyone is driven by a single shared hope: perhaps I know something other doctors haven’t said so far. Maybe there’s a shorter route, maybe more precise, maybe finally a solution.
Tinnitus — commonly called ear ringing or ear noise — is a condition in which you perceive a sound in the ear or head without an external source. It can be a ringing, buzzing, humming, hissing, or even a pulsating sound. It is not an independent disease but a symptom that can have many underlying causes.
If you have just started getting to know home electrotherapy devices, you’ve probably thought: TENS, EMS, MENS, IF, iontophoresis, tVNS, CES, biofeedback – each abbreviation hides very different treatment methods. It’s also a common trap that a multifunction device includes all of them, but the patient does not know which program to use for what.

What do osteoarthritis, insulin resistance, leaky gut and atherosclerosis have in common?
They all share the same silent driver: chronic low-grade inflammation. The good news: diet and daily physical activity are the two most powerful intervention points you can use to fight it.

A cranial electrotherapy stimulation (CES) — in Hungarian, cranial electrotherapeutic stimulation — is a non-invasive, low-intensity electrical neuromodulation typically applied to the ear lobe, forehead, or temple area. The method has historical roots in the 1950s; its modern form was cleared by the US FDA in 1979 — its traditional main indications are the treatment of insomnia, anxiety and depression.

The saddle joint osteoarthritis — professionally called rhizarthrosis or CMC‑I osteoarthritis — is a degenerative condition of the joint at the base of the thumb. This joint lies between the carpal bone called the trapezium and the first metacarpal, and gets its name from its saddle‑like articular surfaces: the two bone ends sit on each other like a saddle on a horse’s back. This unique shape allows you to oppose your thumb to the other fingers — referred to in medical terms as opposition.
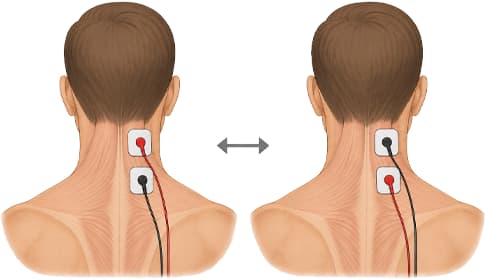
Home electrotherapy devices work with two electrodes: current flows from one (positive, anode) toward the other (negative, cathode). In treatments that use direct (DC, galvanic) current, the two poles have different physiological effects. In alternating-current or biphasic treatments the polarity constantly reverses, so the question is practically meaningless.

Arm swelling after breast cancer treatment – internationally referred to as BCRL (breast cancer-related lymphedema) – is one of the most common long-term complications for patients treated for breast cancer. Clinical practice shows that 20–30% of women who have undergone breast cancer treatment will develop upper-limb lymphedema during their lives – so almost every third survivor. The risk persists for years after surgery and often first appears 2–10 years later.