Forms of electrical muscle stimulation (EMS)
Electrical muscle stimulation (EMS) is a method for treating muscles. There are several forms, each with a different mode of application and, naturally, different effects. Here I present these methods one by one. A little muscle physiology Under normal conditions muscles contract in response to an electrical impulse coming from the brain. The impulse also conveys how forceful the contraction should be and which muscle fibers should contract for a given movement. Obviously, lifting a 1-forint coin and lifting a 100 kg weight require different commands: different fibers and a different muscle mass are involved in the small movement than when maximal force is required.

Electrical muscle stimulation (EMS) is a method for treating muscles. There are several forms, each with a different mode of application and, of course, different effects. I will now introduce these methods one by one.
A little muscle physiology
Under normal circumstances muscles contract in response to an electrical impulse from the brain. The impulse also conveys how forceful the contraction should be and which muscle fibers must contract for a particular movement. It is obvious that the instruction for picking up a small coin differs from that for lifting 100 kg. In the small-weight movement different muscle fibers and a smaller muscle mass participate than when maximal force must be produced.
Muscle strength can be improved by REGULAR physical exercise. Muscles respond to progressively harder training by developing stronger and thicker fibers, which are also more efficient in function.
In many cases natural movement is not possible. Accidents, joint and muscle injuries, severe illnesses, or surgeries can hinder natural movement; inactivity then leads to the opposite process in the muscles, namely atrophy.
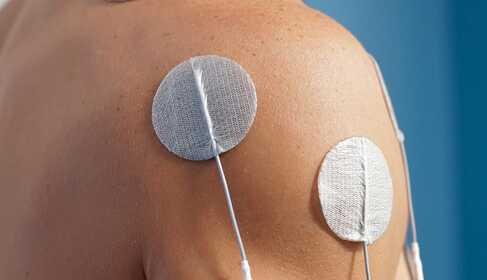
Various forms of electrical muscle stimulation can be used to artificially improve the condition of muscles. The electrical signal delivered by the device is similar to the brain's impulse, so the muscle cannot distinguish between them. Stimulation produces a contraction in the muscle just like a voluntary one. Artificial stimulation has several advantages. First, no joint movement occurs during the treatment, which is beneficial for rehabilitation and for reducing joint load. Second, the artificial impulse can “bypass” the brain's regulation of muscle activity, which can provide a more effective treatment.
Forms of electrical muscle stimulation (EMS)
For all forms of electrical stimulation it is true that contractions are elicited by impulses delivered to the muscle by a device, but the contraction itself occurs naturally. If the contraction is natural, its result will also be the same — with persistent treatment muscle strength, mass and function improve. When muscle strength and function improve, natural movements become easier to perform.
Within muscle stimulation several methods are distinguished. The operating principle is the same, but the shape of the impulse (waveform), its duration, frequency, rise and fall times, and intensity differ. These differences produce different effects.
Strengthening muscles takes time. If a single stimulation produced a significant change, athletes would only use that: tonight I stimulate and tomorrow I go to the Olympics… It's not that simple.
Muscles strengthen only under the influence of regular contractions. Therefore muscle stimulation should be applied at least once daily, preferably several times. Improvements are noticeable after 2–3 weeks and persistent treatment is required for at least 2–3 months.
There are conditions (paralyses) in which application may be necessary for years.
NEMS – Neuromuscular Electrical Stimulation
A method used to treat muscles that have intact motor neurons. This method is also suitable for treating central (brain) paralysis, such as that caused by stroke.
Its main applications are regaining muscle strength, preventing or slowing muscle atrophy, relieving muscle stiffness, improving blood circulation, etc. Different effects require different impulse parameters. One and the same impulse does not produce all effects!
NEMS is the oldest form of muscle stimulation, during which the patient is “passive.” The patient tolerates the treatment but does not actively cooperate with the device, unlike with FES or ETS methods.
It is excellent in all conditions where muscle strength, mass or tone need to be restored or rebuilt — for example muscle atrophy, herniated discs, lumbago, sciatica, varicose complaints, peripheral artery disease, muscle pain, neck/back/low back/knee and other muscle pains. It speeds recovery before and after prosthetic (joint replacement) surgery. It helps relieve muscle stiffness in central paralysis, Parkinson's disease, ALS, multiple sclerosis, etc. It accelerates relearning movement after stroke-induced paralysis.
FES – Functional Electrical Stimulation
Functional electrical stimulation is actually a form of NEMS but requires active cooperation from the person receiving treatment. When the device senses the impulse and the contraction it evokes, the patient simultaneously performs the movement. For example, in the treatment of stress incontinence the pelvic floor muscles are contracted at the same time as the impulse, or when strengthening the thigh muscles the patient performs a squat together with the impulse.
FES has a stronger effect than passive NEMS because the contractions produced by the device and those produced voluntarily add together, resulting in a more powerful contraction and thus a stronger stimulus to the muscle. Consequently, muscle strength increases faster.
Accordingly, FES is primarily used to regain or increase muscle strength. It is especially effective for various forms of urinary and fecal incontinence. It helps restore muscle strength after surgery and serious illness and speeds recovery after prosthetic surgery. In Parkinson's disease, ALS, multiple sclerosis, etc., it slows the deterioration of muscle condition.
ETS – Stimulation triggered by EMG (biofeedback)
This treatment also focuses on restoring function. Like FES, ETS requires cooperation with the device. However, here the device only delivers the muscle stimulation impulse when the patient voluntarily initiates the movement. The device detects this with the help of biofeedback. During a muscle contraction an electrical potential change occurs; the device detects this EMG signal. If the electrical potential change caused by the attempted movement reaches a preset threshold, the device delivers an assisting impulse to produce a contraction. A good ETS device (e.g., DuoBravo) is so sensitive that it can detect activity even when no visible contraction is yet present.
There are two main uses for this triggered stimulation: incontinence treatment and relearning movement after stroke. In the case of stroke it can be used if the patient is cooperative and highly motivated to recover. This is obvious because ETS requires patient activity. ETS can be applied even when there is no visually observable contraction in the paralyzed muscles. Its greatest role, however, is in relearning fine movements (standing up from a chair, grabbing a glass, grooming, etc.).
TES – Threshold Electrical Stimulation
This type of treatment is used for the central (brain) paralysis of children, primarily to prevent and improve muscle atrophy and spasticity.
Threshold electrical stimulation (TES) is a form of muscle stimulation that uses a sub-contraction stimulus. That means the impulse intensity is so low that it does not cause a visible contraction (unlike NMES and FES, where a strong contraction is desired), yet it is still important for the muscle.
The exact mechanism of action is not fully understood. The accepted theory is that TES prevents and reverses muscle atrophy by increasing blood flow to the muscles. Growth factors and nutrients are delivered by the bloodstream; these are necessary for tissue repair. These substances are most effectively mobilized into the bloodstream during sleep. Nighttime stimulation of the muscle area increases blood flow and thus delivers more nutrients to the targeted muscle fibers. The atrophied fibers “repair” themselves and grow.
Under the microscope after TES treatment an increased amount of cytoplasm is visible, along with regrowth of actin and myosin. The regrowth of atrophied fibers lasts about three to six months. Muscle growth requires continuous therapy. TES is typically applied six nights per week, for 8–12 hours per day, for two to four years! The result is increased muscle strength and improved functional abilities.
TES does not replace other therapies but can be used alongside them and considered a complementary treatment.
Treatment of denervated muscle (selective current stimulation)
In Hungary this treatment is traditionally called selective current stimulation. In international medical practice it is called denervated treatment, which better describes what it is.
A denervated muscle means the motor nerve running from the spinal cord to the muscle has been damaged, so the brain–muscle connection is lost. This causes peripheral paralysis, and the denervated muscle becomes flaccid and without tone. Such a condition can result from traumatic or surgical injury to a nerve fiber, but herniated discs, spinal fractures, spinal stenosis, etc. can also cause it. Facial nerve paralysis is another example, although that is often a consequence of a cold.
A denervated muscle does not respond to normal EMS impulses (i.e., to any of the previously mentioned methods)! However, with specially configured impulses it can be induced to contract. The denervated impulse may be triangular, trapezoidal, or square-wave.
The biggest difference is the impulse duration, which is thousands of times longer than that used for stimulating a healthy muscle! Consequently, a denervated muscle cannot contract in response to the short EMS impulse, while for a healthy muscle the long-duration denervated impulse would be painful or uncomfortable.
Recovery from peripheral nerve injury is very slow. Even in fortunate cases it takes many months, and years are more likely. If the muscle is not given electrotherapy during this time, it will deteriorate. Even if the nerve regenerates, it may no longer find a functioning muscle. Therefore in peripheral paralysis the stimulator must be used continuously (even 2–3 times daily).
Muscle stimulator devices available in stores are usually suitable only for NEMS and partially for FES. ETS, TES and denervated treatments are typically available only in devices specifically designed for those purposes. For choosing the right muscle stimulation device for you, seek expert help!