

In this article I explain how TENS fits into multimodal pain management for endometriosis, what home protocols are recommended, and when specialist consultation is absolutely necessary.
 Key point
Key point
The 2020 Brazilian multicenter RCT by Mira et al. (PMID 33129015) found that home TENS added to hormonal therapy produced a meaningful reduction in pelvic pain compared with the control group and improved quality of life and sexual function. The 2025 umbrella review by Tahmasbi et al. (PMID 40626937) identified TENS as one of the consistently supported noninvasive options for chronic pelvic pain. However, TENS does not replace causal medical treatment of endometriosis – it is solely an adjunct for pain relief.
 Types of pain associated with endometriosis
Types of pain associated with endometriosis
For diagnosis and treatment planning it is important to recognise that endometriosis can cause several different types of pain – and these do not respond equally to home measures.
Cramping in the lower abdomen and lower back that intensifies during or just before menstruation. In endometriosis these cramps are typically stronger and longer-lasting than "average" menstrual complaints. The 2022 randomized, double-blind trial by Guy et al. (PMID 35249825) demonstrated rapid onset of effect of TENS for this type of pain: 74% of participants experienced pain relief within <20 minutes, and the effect lasted on average for about 7 hours.
Lower abdominal and pelvic pain that persists for months, independent of the menstrual cycle. The 2025 umbrella review by Tahmasbi et al. (PMID 40626937) concluded that TENS and PTNS (percutaneous tibial nerve stimulation) are among the best-supported noninvasive options for managing chronic pelvic pain; these treatments are generally well tolerated and rarely cause adverse effects.
Deep pelvic pain felt with deep penetration – particularly common in endometriosis and significantly impairing quality of life. The 2025 scoping review by Cook et al. (PMID 40846214) identified TENS, botulinum toxin, and pelvic physiotherapy as the most promising treatment directions – but all cases require specialist evaluation.
Pain during bowel movements or urination, typically worsening around menstruation. These may indicate bowel or bladder involvement by endometriotic lesions and require specialist evaluation – TENS alone is not suitable to manage these conditions.
Multimodal pain management – the role of TENS
Treating endometriosis pain usually achieves meaningful improvement through combining multiple methods. In the 2020 Mira et al. trial, the combination of hormonal therapy + TENS produced a meaningful reduction in pelvic pain compared with hormonal therapy alone; thus TENS complements rather than replaces causal treatment. The full range of approaches:
| Approach | What it helps with | Limitations / notes |
|---|---|---|
| Hormonal therapy (by physician) | Suppression of endometriotic tissue, ovulation suppression | Foundation of pain management, but has side effects (mood, libido, bone density) |
| NSAIDs (e.g. ibuprofen) | Acute prostaglandin-mediated pain (cramps) | Regular use can cause gastrointestinal side effects – consult your treating physician |
| Heat therapy (heating pad, bath) | Relieves spasms, muscle relaxation | Short-term effect, often needs repeated application |
| TENS (home electrotherapy) | Chronic pelvic pain, dysmenorrhea cramps | Adjunctive, does not replace causal treatment; watch for contraindications |
| Pelvic physiotherapy / rehabilitation | Pelvic floor muscle rehabilitation, dyspareunia | Requires a specialised pelvic physiotherapist |
| Lifestyle: regular exercise, stress management | Reduces general pain sensitivity | Time-consuming, requires long-term commitment |
In the remainder of this article I present a detailed home protocol for using TENS – the other methods should be integrated into the comprehensive treatment plan in consultation with your treating physician or physiotherapist.
 Why and how TENS affects endometriosis pain
Why and how TENS affects endometriosis pain
TENS delivers small electrical impulses through the skin to sensory nerves. It can relieve pelvic pain via two main mechanisms:
- Conventional (gate control) effect: high-frequency (50–150 Hz) impulses act on Aβ fibres to "close the gate" in the dorsal horn of the spinal cord, preventing pain signals from reaching the brain. The effect is rapid (within minutes) and typically lasts 1–3 hours during and after treatment.
- Endorphin TENS effect: low-frequency (2–10 Hz) impulses can stimulate release of endogenous opioids (endorphins, enkephalins). This effect starts more slowly (15–30 minutes) but can last longer, even 4–8 hours.
The two programs can be combined: during the day use short, fast-acting conventional TENS for acute painful episodes, and in the evening or before bed use longer endorphin TENS to reduce baseline pain. If your device supports it, a modulated program (continuously varying parameters) helps maintain effectiveness with repeated use by reducing habituation. Details: TENS programs.
 Home TENS protocol for endometriosis
Home TENS protocol for endometriosis
Minimum equipment for home use:
- 1 two-channel TENS or TENS+EMS device (CE/MDR-certified medical device)
- 2 stimulation cables
- 4 self-adhesive TENS electrodes (5×5 cm is the most common and comfortable size)
Electrode placement
The figure below shows the two most commonly used placements. Both are suitable for TENS treatment – try both and keep the one that feels more comfortable and effective for you.
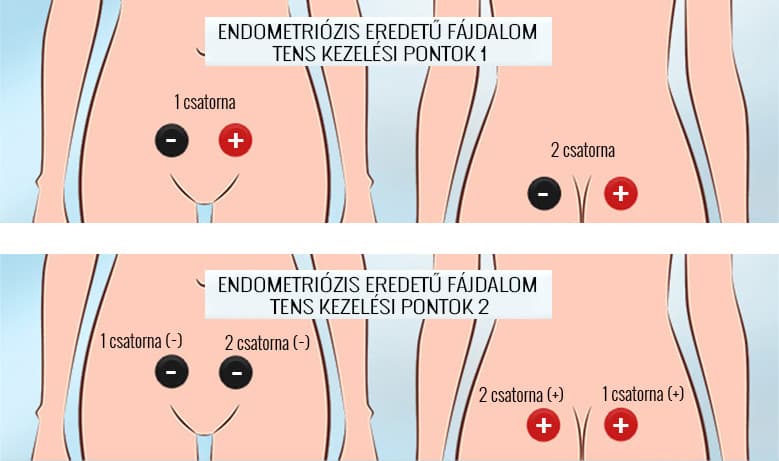
- Variant 1 – front and back: the two electrodes of CH1 are placed on the lower abdomen (on either side of the line below the navel), and the two electrodes of CH2 are placed symmetrically above the sacrum on the back.
- Variant 2 – diagonal: for CH1 place one electrode on the front right lower abdomen and the other on the right sacral area at the back. Connect CH2 in the same diagonal pattern on the left side.
- The two electrodes belonging to the same channel should always lie on the same stimulation pathway.
- Never place an electrode directly on the spine, over the sternum, or on the head.
Program selection and intensity
- For cramping, acute pain: conventional TENS (typically 80–120 Hz, a fine tingling sensation, no muscle twitching).
- For chronic, baseline pain or evening relaxation: endorphin TENS (2–10 Hz, rhythmic, mild muscle twitching).
- For long-term use and habituation prevention: modulated program.
- Increase current gradually from zero; the aim is a pleasant, definite tingling (or a mild twitch for endorphin TENS), but never a painful sensation. Details: TENS programs.
Treatment duration and frequency
- A single session typically lasts 20–30 minutes (study protocols range from 20 to 60 minutes).
- Use 2–3 times daily for regular application; add extra sessions during acute spasms.
- The 2020 Mira trial found clinically significant quality-of-life improvements after an 8-week home use period.
- Take 1–2 days off per week to reduce the risk of habituation.
If pain is particularly strong before or during menses, it is worth starting treatment preventively – begin when symptoms start to intensify rather than at the pain peak. Many patients find this approach substantially improves comfort.
When should TENS NOT be used in endometriosis?
TENS is generally a well-tolerated adjunct, but in some situations home use is not recommended or requires specialist supervision. The full contraindication list can be found in the electrotherapy contraindications article.
- Pregnancy (or suspected pregnancy) – lower abdominal TENS is not recommended; only use after specialist consultation and not with lower abdomen–sacrum placement.
- PACEMAKER, defibrillator (ICD) or other implanted electronic device – details: implants and electrotherapy.
- New, unexplained lower abdominal pain – specialist evaluation is recommended first.
- Suspected bowel or bladder involvement (blood in stool or urine) – urgent medical assessment.
- Skin inflammation, wounds, or fresh surgical incisions in the treatment area.
- Suspected or known pelvic malignancy – details: cancer-related considerations.
- Epilepsy (TENS is generally safe, but consult a specialist for new or unstable cases).
When should you definitely see a doctor?
Causal treatment of endometriosis (hormonal therapy, possibly surgery) is exclusively the responsibility of specialists. Home TENS use is only adjunctive. Seek a gynaecologist or other specialist in the following situations:
- New-onset, qualitatively different lower abdominal pain (especially if previous pain is now different from usual)
- Sudden, severe, extraordinary pain (possible ovarian cyst rupture or other emergency)
- Fever, chills, or general malaise accompanying lower abdominal pain (suggesting infection)
- Blood in stool or urine
- Unintentional weight loss, loss of appetite
- Persistent, worsening pain despite home measures
- Suspected endometriosis that has not yet been evaluated by a specialist
Your treating physician can determine, based on history, physical examination and (if needed) ultrasound or MRI, whether home TENS can be used safely for your condition.
 Summary – key takeaways
Summary – key takeaways
- According to recent (2020+) clinical trials, TENS can meaningfully reduce endometriosis-related pain when used as an adjunct – it does not replace causal treatments.
- Conventional TENS (60–120 Hz, gate control) provides rapid relief; endorphin TENS (2–10 Hz, opioid-mediated) offers longer-lasting effects.
- Home protocol: two-channel device, four 5×5 cm electrodes, lower abdominal + sacral placement, 20–30 minute sessions, 2–3 times daily.
- TENS does not replace hormonal therapy, physiotherapy, NSAIDs or specialist follow-up.
- Do not use at home if pregnancy is suspected, you have a pacemaker, new unexplained pain, or blood in stool/urine—seek medical attention instead.
Entry-level home choice: Dolito TENS – simple, compact, focused on pain relief. Detailed device selection guide: Choosing a TENS device.
 Frequently asked questions
Frequently asked questions
TENS can reduce the amount of analgesics needed for many patients – the 2022 study by Guy et al. (PMID 35249825) reported about a ~93% reduction in analgesic use for primary dysmenorrhea. However, this is individual: TENS cannot be said to universally replace medications. Any medication changes should always be discussed with your treating physician.
Yes, this is precisely the time when TENS provides the greatest help for most patients. Lower abdominal and sacral placements are the most common. Avoid placing electrodes directly over the uterus or using intensities that provoke strong muscle contractions – stay in the gentle, pleasant tingling range.
TENS targets sensory nerves with low-intensity stimulation to relieve pain; EMS, by contrast, uses higher amplitude to stimulate motor nerves and elicit true muscle contractions. EMS is NOT appropriate for endometriosis – cheap muscle stimulators applied to the lower abdomen may be contraindicated. Always choose a CE/MDR-certified device with genuine TENS functionality. More details: Differences between TENS, EMS, MENS.
Generally there is no contraindication while trying to conceive, but it is reasonable to pause treatment after ovulation if your period is delayed and wait until the next menstruation to resume. If pregnancy is confirmed, consult your gynaecologist – lower abdominal–sacral TENS is generally not recommended during pregnancy.
The 2022 study by Guy et al. (PMID 35249825) reported that 74% of participants experienced relief within <20 minutes. The 2020 Mira trial (PMID 33129015) found that clinically significant reduction in chronic pelvic pain developed with regular use over 8 weeks. These two dimensions complement each other: rapid relief during an episode plus gradual baseline reduction with long-term use.
TENS is generally well tolerated; the 2025 umbrella review by Tahmasbi et al. (PMID 40626937) also rated it as having "minimal, tolerable side effects." The most common complaint is mild skin redness or irritation under the electrode – usually prevented by moving the electrode or properly cleansing the skin. Incorrect intensity can cause unpleasant sensations or rarely muscle cramps – reduce current in that case.
Related articles
Scientific sources (2020+)
- Mira TAA, Yela DA, Podgaec S, Baracat EC, Benetti-Pinto CL. Hormonal treatment isolated versus hormonal treatment associated with electrotherapy for pelvic pain control in deep endometriosis: Randomized clinical trial. European Journal of Obstetrics, Gynecology, and Reproductive Biology. 2020 Dec;255:134-141. DOI: 10.1016/j.ejogrb.2020.10.018 · PMID: 33129015
- Guy M, Foucher C, Juhel C, Rigaudier F, Mayeux G, Levesque A. Transcutaneous electrical neurostimulation relieves primary dysmenorrhea: A randomized, double-blind clinical study versus placebo. Progres en Urologie. 2022 Jul;32(7):487-497. DOI: 10.1016/j.purol.2022.01.005 · PMID: 35249825
- Tahmasbi F, Rahimi-Mamaghani A, Soleimanzadeh F, Ghaderi S, Aletaha R, Salehi-Pourmehr H, Sedigh O, Mohammad-Rahimi M. Nonimplantable Peripheral Electrical Stimulation for Management of Chronic Pelvic Pain: An Umbrella Review. Neuromodulation. 2025;28(8):1341-1353. DOI: 10.1016/j.neurom.2025.05.009 · PMID: 40626937
- Cook E, Yunker A, Walden RL, Barrett-Chan E, Dhillon H, Gentles A, Sreya M, Zhu W, As-Sanie S, Yong PJ. Female Dyspareunia and the Relationship to Neurophysiologic Mechanisms: A Scoping Review. Journal of Minimally Invasive Gynecology. 2025;33(1):34-59. DOI: 10.1016/j.jmig.2025.07.018 · PMID: 40846214

This article provides general information and does not replace specialist gynaecological consultation. Diagnosis and causal treatment of endometriosis (hormonal or surgical therapy) fall exclusively within specialist competence. Home TENS treatment is an adjunctive pain-relief method – always discuss its use with your treating physician, especially if you are planning pregnancy, are pregnant, taking medications, or have an implanted medical device. TENS devices are CE/MDR-certified medical devices – follow the user manual.