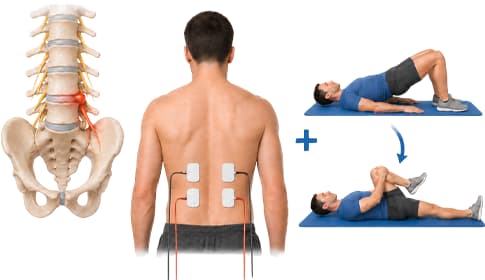

 If you have a disc herniation, use EMS alongside physiotherapy
If you have a disc herniation, use EMS alongside physiotherapy
You sit hunched at the computer all day, then sway in traffic and can’t wait to collapse into your armchair and watch your favorite series. Your physical activity is close to zero — no wonder your back starts to hurt. The more you rest, the more it hurts. The more it hurts, the less you move. It all leads to one vicious cycle: the weakening of the spinal stabilizing muscles, especially the deep (paraspinal) stabilizers. These are nearly impossible to reach with voluntary exercises alone — but with intact nerve supply an electrical stimulator (EMS) can “prime” them, i.e., pre-activate them.
 Key point
Key point
The key to disc herniation rehabilitation is reactivating the deep spinal stabilizers (multifidus, transversus abdominis). These muscles are barely targeted during painful phases of exercise — EMS, however, directly elicits muscle contraction regardless of how much voluntary "will" is behind it. Exercise + EMS together produce measurably more than either alone.
Why does a disc herniation hurt, and why doesn't it resolve by itself?
A disc herniation develops when the elastic nucleus of the intervertebral disc breaches the outer fibrous ring under intermittent or sustained loading. The protruding material can press on nerves — this causes the classic radiating pain (sciatica), numbness or muscle weakness in the leg.
Many patients are surprised to learn that pain does not arise solely from the disc abnormality itself, but from the loss of the protective power of surrounding muscles. The deep muscles around the painful area — mainly the multifidus and transversus abdominis — are poorly activated due to pain inhibition, become shortened and stiff. This creates a relative muscle weakness: although someone may appear fit externally, their deep stabilizers can be compromised.
 Even manual workers complain
Even manual workers complain
Often manual workers or bricklayers seek help for back pain. Their spinal stabilizers are clearly stronger than those of office workers. Still, constant heavy lifting — especially with poor technique — can produce a “relative muscle weakness”: their deep stabilizers do not keep pace with the surface muscles.
 How can EMS help in spinal rehabilitation?
How can EMS help in spinal rehabilitation?
Electrical therapy can play three distinct roles in disc rehabilitation. Each serves a different purpose and requires different settings.
EMS – reactivating the deep stabilizers
EMS (Electrical Muscle Stimulation) stimulates the motor nerve fibers of the muscle, causing muscle contraction — even when you can barely move voluntarily because of pain. With paraspinal electrode placement the current reaches not only surface muscles but, according to studies, significantly activates the deep stabilizers (multifidus, transversus abdominis, internal oblique).1
This “neurological priming” effect is particularly important after the acute phase when pain has caused the deep muscles to “forget” how to activate. Stimulation wakes them up — from there exercise becomes much more effective.
TENS – pain relief so exercise can be performed
TENS (Transcutaneous Electrical Nerve Stimulation) stimulates sensory nerve fibers and thus blocks pain signals to the brain (gate theory). Radiating sciatic-type pain and sharp low back pain can be reduced with it.
In a 100-patient disc herniation–sciatica trial, electrical stimulation reduced pain more effectively (on several pain scales) than conventional traction treatment.5 Important: TENS has no effect on muscle strength or function4 — therefore use TENS before exercise to reduce pain, but TENS alone is insufficient for lasting improvement.
EMS + exercise – the proven better combination
The best results are achieved when the two methods are combined. Studies show that coordinated, parallel application of NMES stimulation and voluntary movement produced measurably better deep muscle activation and greater muscle hypertrophy than exercise or stimulation alone.3
A comprehensive 2023 review found that EMS (and especially EMS + exercise) was more effective than passive and active controls for trunk muscle endurance and strength in chronic low back pain.6 The logic is simple: EMS “starts” the muscle, and exercise teaches you how to use it in daily movement.
Why is physiotherapy alone not always sufficient?
Physiotherapy is the foundation of disc herniation rehabilitation — but for the reasons below it is often slow or insufficient on its own. This is why adding EMS can be worthwhile:
| Problem | Why is it difficult? | How EMS contributes |
|---|---|---|
| Too short, too infrequent | One or two physiotherapy sessions per week are insufficient to build lasting muscle strength. | Daily 20–30 minute home stimulation greatly multiplies the muscle workload. |
| Pain prevents exercise | Because of pain you don't dare to challenge your muscles — you unknowingly “protect” them. | EMS elicits contraction even without producing joint movement, so it does not provoke pain. |
| Deep muscles do not activate | The multifidus and transversus abdominis are difficult to activate voluntarily — exercises mainly recruit surface muscles. | Paraspinal electrode arrangements directly activate the deep stabilizers.1 |
| Lack of motivation and persistence | Maintaining months of weekly exercise is hard to sustain. | The home device is convenient — it can be used while watching TV, as part of an evening routine. |
 EMS does not replace exercise in the long term!
EMS does not replace exercise in the long term!
EMS “starts” the deep muscles — but only voluntary exercise teaches everyday movements (walking, climbing stairs, lifting). The ideal ratio: use EMS more intensively in the initial weeks; as exercise is progressively integrated, stimulation becomes a supplementary tool.
For which spinal problems is EMS worthwhile?
The most typical indication. After the acute painful phase has subsided — in the subacute or chronic stage — it is worth starting. Combined EMS + exercise usually shows visible improvement in pain, range of motion and function after 8–12 weeks. A randomized clinical trial found that stimulation combined with movement produced better outcomes in sciatica patients within 8 weeks.4
In degenerative disc disease the disc loses its elasticity. Surgery is only a last resort — meanwhile targeted muscle stabilization (paraspinals and core) slows the process. EMS helps prevent compensation by surface muscles alone.
Due to radiating leg pain, exercise is difficult to perform — here TENS can provide a pain block so you can do the exercises while EMS works on the stabilizers. Clinical trials confirm that electrical stimulation is superior to passive traction controls for sciatica pain relief.5
After disc surgery, spinal stabilizers waste rapidly due to movement restriction. McKenzie extension exercises combined with NMES reduce pain scores and functional disability points.8 Always obtain your surgeon's approval post-op and start with gentle intensity.
After hospital or physiotherapy programs end, strength gains can decline within weeks. Home EMS alongside exercise can maintain the rebuilding phase for months.
 Home EMS devices for spinal rehabilitation
Home EMS devices for spinal rehabilitation
For spinal rehabilitation you need a 4-channel device that can stimulate the posterior and abdominal musculature simultaneously. One clinical trial specifically found this arrangement most effective for activating the deep stabilizers.2
 My advice on program selection
My advice on program selection
Three program groups are useful for spinal rehabilitation: Warm-up / stiffness release (5–10 minutes, low frequency) before exercise; Strength / muscle tone (20–30 minutes, 30–50 Hz) targeting deep muscles; Active recovery / massage (10–15 minutes, 1–8 Hz) after exercise. For the detailed 12-week protocol see the 4-channel back strengthening program plan →
 Before you start home EMS treatment
Before you start home EMS treatment
The following situations are contraindications for using a lumbar stimulator or require specialist consultation:
- Acute inflammatory phase with strong radiating pain – first reduce the pain, then start stimulation.
- Implanted pacemaker, ICD, spinal cord stimulator or other active implant – the current may interfere with device function.
- Pregnancy – abdominal and lumbar electrode arrangements are not recommended.
- Cancer in the treatment area – avoid the affected region.
- Fresh surgical area – wait for wound healing (minimum 2–3 weeks) and start only with medical approval.
- Skin disease, injury or sensory loss in the treatment area – the skin should be intact and sensitive.
- Epilepsy or other seizure disorders – stimulation can be a trigger.
- Deep vein thrombosis or active vascular occlusion – the current may worsen the condition.
- Acute fever or infectious illness – wait for recovery.
- Severe cardiovascular disease – request cardiology approval in case of arrhythmia or heart failure.
Consult your treating physician
Disc herniation is a complex condition. Home EMS treatment does not replace medical diagnosis and protocol — always obtain approval from your treating physician, physiotherapist or rehabilitation specialist before starting. For the full contraindication list, read our electrical therapy contraindications article.
 What does the science say about using EMS in spinal rehabilitation?
What does the science say about using EMS in spinal rehabilitation?
Clinical trials consistently support the role of EMS in disc herniation rehabilitation. Some key data:
“Does EMS really reach deep muscles that exercise can't?”
Yes. In an ultrasound imaging study, NMES applied to the paraspinal area significantly activated the deep stabilizers — multifidus, transversus abdominis, internal oblique — which are often “unreachable” with voluntary exercise alone.1
“What is the ideal electrode arrangement for spinal strengthening?”
Simultaneous abdominal + posterior (4-channel) placement proved superior for activating deep muscles compared with posterior-only or abdominal-only arrangements. The combined protocol produced significantly greater hypertrophy in both multifidus and abdominal stabilizers.2
“What changes when I add EMS to exercise?”
In a 2021 clinical trial, NMES added to motor control exercises produced measurably greater multifidus activation in patients with recurrent low back pain than pseudo-stimulation. Stimulation acts as a “neurological priming”: it wakes the muscle so exercise can use it effectively.3
“Is TENS alone enough, or is motor control exercise necessary?”
A 2019 study in patients with disc herniation and radiculopathy found that after 8 weeks motor control exercise produced significantly better results than TENS alone on pain and function scales, and increased transversus abdominis activation.4
“What do systematic reviews show?”
A large 2023 systematic review and meta-analysis concluded that NMES (and especially EMS + exercise) was superior to passive and active controls for trunk muscle endurance and strength in chronic low back pain. The evidence consistently supports the combined approach.6
“Can a young or athletic person benefit?”
Yes. In a 2023 clinical trial of 128 active-duty military personnel with subacute low back pain, NMES strengthening therapy improved physical performance (sit-to-stand, push-ups) and trunk strength more than standard care — demonstrating a dose–response relationship.7
The gist
Scientific evidence is consistent: EMS effectively reaches deep stabilizers that exercise poorly targets. Combined EMS + exercise produces greater muscle activation, hypertrophy and functional improvement than exercise alone. Significant effects appear after 8–12 weeks of regular use.
How to integrate EMS into rehabilitation?
Principles of EMS treatment in disc herniation
- Acute phase (weeks 1–2): if you have strong radiating pain, first aim to reduce pain. TENS program (80–150 Hz, gentle tingling) at low intensity for 20 minutes. Do not stimulate the lumbar area if there is a strong acute inflammatory reaction!
- Subacute phase (weeks 3–6): begin muscle priming. Warm-up or “stiffness release” program (5–10 minutes), then “Strength / muscle tone” program (20–30 minutes, 30–50 Hz) on paraspinal and abdominal areas.
- Chronic phase (weeks 7–12 and beyond): exercise becomes primary, EMS in a supplementary role 3–4 times weekly. Progress intensity gradually.
- Electrode placement: 2–3 cm lateral to the spinous processes (over the paraspinal muscle band), vertically aligned. With a 4-channel device also place electrodes simultaneously over the transversus abdominis.2
- Intensity: above sensory threshold, gradually increased to visible contraction. Always stay below pain threshold!
- Duration: 1 (or 2) sessions daily of 20–30 minutes. 4–6 sessions per week.
- Timing relative to exercise: EMS "Warm-up" → 30–60 minute rest → exercise; or use an "Active recovery" program after exercise.
Maintenance — preserving the result
- After week 12, exercise should be the base (3–4 times weekly), with EMS as maintenance 1–2 times weekly.
- Ergonomics (chair setup, monitor height, lifting technique) are equally important — without them even strengthened muscles can be overloaded.
- NSAID painkillers (Algoflex, ibuprofen, Nurofen etc.) provide symptomatic relief but have long-term side effects — they do not replace muscle strengthening. The exercise + EMS approach addresses the problem at its source.
Frequently asked questions
Start after the acute, strongly radiating painful phase — usually after 2–3 weeks when pain is tolerable. In the first 1–2 weeks rest and gentle pain management are primary. Always get your treating physician's approval before starting.
The first noticeable changes (less stiffness, better support, less fatigued lower back) appear after 2–3 weeks of regular EMS + exercise. Measurable muscle hypertrophy and functional improvement stabilize after 8–12 weeks.3, 6
No. EMS “starts” the deep muscles, while physiotherapy teaches you how to use them in everyday movements. The two together deliver more than either alone. Physiotherapy is the long-term solution; EMS supports faster recovery.
During the rebuilding phase (months 1–3) use it 4–6 times weekly, 20–30 minutes daily. In the maintenance phase (from month 3) 1–2 times weekly is sufficient if you continue to exercise regularly.
After disc surgery (discectomy) you can generally start gentle EMS around 2–3 weeks post-op with surgical approval — after normal wound healing and scar formation. McKenzie extension exercises combined with NMES favorably support recovery.8
With a 4-channel device you can simultaneously stimulate the posterior paraspinals (2 channels) and the abdominal stabilizers (transversus abdominis — 2 channels). Clinical trials found this simultaneous combined arrangement most effective for deep muscle activation.2 A 2-channel device can achieve the same only in separate stages, which doubles the time and provides less synchronized muscle activation.
 Summary – Quick overview
Summary – Quick overview
Sources
- Baek SO, Ahn SH, Jones R, Cho HK, et al. (2014). Activations of deep lumbar stabilizing muscles by transcutaneous neuromuscular electrical stimulation of lumbar paraspinal regions. Annals of Rehabilitation Medicine 38(4):506-513. PubMed: 25229029
- Kim SY, Kim JH, Jung GS, Baek SO. (2016). The effects of transcutaneous neuromuscular electrical stimulation on the activation of deep lumbar stabilizing muscles of patients with lumbar degenerative kyphosis. Journal of Physical Therapy Science 28(2):399-406. PubMed: 27064323
- Songjaroen S, Sungnak P, Piriyaprasarth P, Wang HK. (2021). Combined neuromuscular electrical stimulation with motor control exercise can improve lumbar multifidus activation in individuals with recurrent low back pain. Scientific Reports 11(1):14815. PubMed: 34285318
- França FJR, Callegari B, Ramos LAV, Burke TN. (2019). Motor Control Training Compared With Transcutaneous Electrical Nerve Stimulation in Patients With Disc Herniation With Associated Radiculopathy: A Randomized Controlled Trial. American Journal of Physical Medicine & Rehabilitation 98(3):207-214. PubMed: 30247159
- Wang L, Fan W, Yu C, Lang M, Sun G. (2018). Clinical effects of electrical stimulation therapy on lumbar disc herniation-induced sciatica and its influence on peripheral ROS level. Journal of Musculoskeletal & Neuronal Interactions 18(3):393-398. PubMed: 30179218
- Wolfe D, Rosenstein B, Fortin M. (2023). The Effect of Transcutaneous Electrotherapy on Lumbar Range of Motion and Paraspinal Muscle Characteristics in Chronic Low Back Pain Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine 12(14):4680. PubMed: 37510796
- Talbot LA, Webb L, Ramirez VJ, Morrell C, et al. (2023). Neuromuscular electrical stimulation for the management of subacute low back pain: a randomized controlled trial in active-duty military personnel. Military Medicine 188(1-2):12-19. PubMed: 34510214
- Abdi A, Bagheri SR, Shekarbeigi Z, Usefvand S, Alimohammadi E. (2022). The effects of McKenzie-based exercises on outcomes in patients with lumbar disc herniation following discectomy: a randomized clinical trial. Neurological Research 45(1):28-40. PubMed: 36039973
