
 Herniated Disc – what can you do at home to avoid surgery?
Herniated Disc – what can you do at home to avoid surgery?
A herniated disc (correct term: intervertebral disc herniation) is a classic civilization ailment: prolonged sitting, lack of movement and occasionally excessive physical load together place too much strain on the disc, and eventually the outer fibrous ring that contains the jelly-like nucleus can tear. The good news: many people experience a herniated disc, but surgery is not necessary for everyone.
Most people affected do not know what they can do at home to avert the pain and the threat of surgery. This pillar article is for them: I will guide you through home-usable treatment options – from muscle stimulation and softlaser to the foam-roller – and help you decide which method suits which complaints best.
 Key idea
Key idea
International professional guidelines (including the American College of Physicians' 2017 recommendation) state that conservative (non-surgical) treatment is the first-line solution for disc herniation – surgery is required only if there is marked neural injury (paralysis, sensory loss, urinary/fecal dysfunction) or if 6–12 weeks of sustained conservative treatment has produced no improvement.2, 3 You can do a lot for your recovery at home.
What you need to know about disc herniation
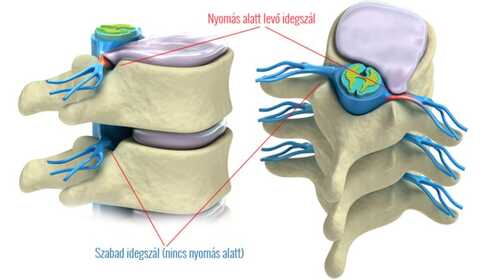
Your spine is built from individual vertebrae with flexible intervertebral discs between them. The disc consists of an outer fibrous ring and a jam-like gelatinous nucleus contained within. If it is exposed to excessive and repeated load (prolonged sitting, improper lifting, overweight, weak spinal-supporting muscles), the fibrous ring can weaken or tear, allowing the gelatinous nucleus to protrude – this is called a disc herniation (hernia disci intervertebralis).
The protruding material can press on surrounding nerves and trigger inflammatory processes there – this causes the classic pain, radiating sciatica, numbness, and sometimes muscle weakness.
 How big is this problem globally?
How big is this problem globally?
Low back pain affects an estimated 577 million people worldwide at any given time (about 7.5% of humanity) and remains the leading cause of years lived with disability.1 You are not alone – and science pays serious attention to effective home solutions.
The most common symptoms of a herniated disc:
- Sharp, stabbing pain in the lower back or neck area
- Radiating pain to the arm (cervical herniation) or leg (lumbar herniation – sciatica)
- Numbness, burning sensation in the affected area
- Muscle weakness in the affected limb
- Pain worsened by coughing or sneezing (increased intra-abdominal pressure)
When should you seek urgent medical attention?
Home treatment does not replace medical diagnosis and protocols. Most herniated discs can be managed conservatively, but certain symptoms may require immediate medical care:
 Red flags – DO NOT wait, DO NOT self-treat
Red flags – DO NOT wait, DO NOT self-treat
- Sudden onset of paralysis or severe muscle weakness (e.g. foot drop)
- Urinary or fecal incontinence (loss of control)
- “Saddle” numbness – loss of sensation around the anus or genital area
- Unbearable pain that does not improve with medication
- Fever accompanying the symptoms
These may be signs of cauda equina syndrome, which can require urgent surgical intervention.
If you only have persistent but tolerable pain and your treating physician recommends conservative therapy, you made the right decision to start looking for home solutions. You can read about these in detail in the following sections.
What home treatment options are available?
The six technologies below can all be used at home. Each has a different primary role – some reduce pain, some decrease inflammation, some strengthen muscles. The best results are usually achieved by combining 2–3 methods. Review them and find which fits your complaint:
Main role: reactivating and strengthening the deep spinal stabilizers (multifidus, transversus abdominis) – even when pain makes conventional exercise difficult.
When to use? Chronic low back pain, disc herniation rehabilitation, subacute–chronic phases of sciatica, post-operative recovery, sarcopenia, muscle weakness due to sedentary work.
Timing of results: first meaningful improvement in 2–3 weeks; muscle hypertrophy after 6–12 weeks of regular use. Should be combined with exercise when possible.
Detailed clinical evidence and protocol → EMS + physiotherapy in disc herniation rehabilitation
Specific 12-week program → Back strengthening with a 4-channel stimulator
Main role: reduce inflammation and edema around the herniated disc – the primary source of pain. The ACP 2017 recommendation and a 2024 international expert consensus also recommend it for low back pain.4
When to use? Acute and chronic low back pain, lumbar discogenic radiculopathy (sciatica), cervical disc herniation, postoperative inflammatory phase.
Timing of results: noticeable pain reduction after 10–14 days of regular (1–3× daily) treatment. Cumulative, gradual effect. Does not eliminate the herniation itself.
Protocol, devices and treatment guide → Softlaser for disc herniation and low back pain
Main role: electrical blockade of pain-conducting nerve fibers – based on the “gate control” theory. Effects are felt within minutes and can last for hours after the session.
When to use? Acute painful episodes, flares of chronic low back pain, painful phases of sciatica, to enable you to perform physiotherapy exercises.
Timing of results: immediate (during treatment). A meta-analysis summarizing 381 clinical trials found moderate evidence that high-intensity non-painful TENS reduces pain intensity compared to placebo.6
Important: TENS is symptomatic treatment – it reduces pain but has no structural healing effect. For chronic use, choose a TENS program that delivers modulated impulses (variable frequency/width) so the nervous system does not habituate.
Detailed guide → TENS therapy – drug-free pain relief
Main role: low current (microampere range) supports cellular ATP production and tissue regeneration. The effect is not felt during treatment – a ‘‘no-intervention’’ sensation.
When to use? Chronic, slow-healing pain where regeneration is the goal; inflammatory conditions (such as edema around a herniated disc); low back pain alongside joint complaints.
Timing of results: regular use for 2–4 weeks. Slower than TENS, but with more structural effects.
Detailed guide → Microcurrent therapy (MENS) – cellular regeneration
Main role: gently heats deeper tissues, improves blood flow, relaxes tense muscles and helps resorb edema.
When to use? Persistently tight, spasmodic back muscles; chronic, deeper low back pain; muscle spasm; slowly healing soft tissue injuries.
Important: do NOT use ultrasound directly over the spine – apply it to the paraspinal muscles on both sides only.
Detailed guide → Therapeutic ultrasound for home use
Main role: mechanical release of stuck, spasmotic muscles. A self-massage alternative to hands-on therapy.
When to use? Muscle soreness, cramps, stuck upper back muscles, pre-/post-treatment regeneration, neck stiffness.
Important: do not use the SMR roller directly over the spine. In acute, severe painful phases be gentle or avoid use.
Detailed guide → What is an SMR roller and how does it help recovery?
Which method for which complaint? – Quick decision aid
If you are still unsure which technology to start with, the table below makes the choice easier. It applies to situations without red flags and suitable for home treatment:
| If your complaint is… | Try primarily | As a supplement |
|---|---|---|
| Recently started, severe sharp pain | TENS (rapid relief) | Softlaser (inflammation reduction) |
| Chronic, "always painful" low back pain | EMS + exercise (muscle strengthening) | Softlaser, MENS |
| Sciatica radiating to the leg | Softlaser (inflammation reduction) | TENS for acute pain, EMS long-term |
| Cervical herniation, shoulder pain | Softlaser + EMS | TENS, foam-roller for the upper back |
| Stuck, spasmodic muscles | SMR roller + ultrasound | Softlaser for deeper inflammation |
| Postoperative rehabilitation | EMS (with medical approval) | Softlaser at a gentle dose |
| Prevention (no herniation yet, but predisposed) | EMS back strengthening | SMR roller for regular mobilization |
 My advice – don’t let it progress to a hernia!
My advice – don’t let it progress to a hernia!
Regular exercise + EMS-based muscle strengthening is most effective when started before a herniation occurs. A weekly routine of 3–4× 20–30 minutes of spinal exercises and 2–3× EMS sessions can protect you from spinal complaints for a long time. If pain has already started, begin home treatment as soon as possible.
 Device categories for home treatment of disc herniation
Device categories for home treatment of disc herniation
To choose the right device, first pick the technology (based on the decision aid above), then find specific device recommendations in the detailed spoke articles:
Muscle stimulators (EMS / TENS / NMES)
4-channel central units for strengthening spinal-supporting muscles: Globus Premium 400, Genesy 300 Pro, MyoBravo, and the Sport Pro line. One device with many programs: strengthening, pain relief, regeneration.
Softlaser devices (LLLT)
808 nm wavelength devices for inflammation and edema reduction: Personal Laser L400, B-Cure Laser Pro, Energy Laser L500 Pro, Energy Laser L2000. From entry-level to professional.
Microcurrent devices (MENS)
For cellular-level regeneration: Dolito, Myolito, Rehalito MTR+ line devices. Choose when chronic regeneration is the main goal.
Therapeutic ultrasound devices
For deep heating: SonicRelief, MediSound 3000. Suitable for home use.
SMR roller
For self-massage and muscle spasm relief. The most affordable entry point – can be integrated into any serious rehab package.
 Before you start home treatment
Before you start home treatment
In the general situations below any electrotherapy or softlaser treatment is contraindicated or requires specialist consultation. Detailed, technology-specific contraindications are in the spoke articles.
- Acute, severe radiating pain – begin treatment only after pain has decreased.
- Suspicion of cauda equina syndrome – urgent medical care, not home treatment.
- Implanted pacemaker, ICD or other active implant – electrical therapies (EMS, TENS, MENS, ultrasound) are forbidden nearby.
- Pregnancy – abdominal and lower back treatment is prohibited.
- Active malignancy in the treatment area – avoid the affected region.
- Fresh surgical area – wait for wound healing (minimum 2–3 weeks) and start only with medical approval.
- Skin disease, injury or sensory loss at the treatment site – the skin must be intact and sensory.
- Epilepsy or other seizure disorders – stimulation can be a trigger.
- Acute fever or infectious illness – wait for recovery.
- Severe cardiovascular disease – seek cardiology approval in case of arrhythmia or heart failure.
Further reading
For the full contraindication list read our electrical treatment contraindications article. For softlaser-specific considerations see softlaser therapy contraindications.
 What does research say about conservative treatment?
What does research say about conservative treatment?
Science gives a clear answer to the “what can you do alone” question. Some important data:
“Do not everyone need surgery?”
A 2024 systematic review (15 trials) found that conservative treatment often provides immediate symptomatic relief for disc herniation, and surgery should be reserved for patients with marked neural injury or those who do not improve with conservative care.2 A 2021 network meta-analysis (32 RCTs, 4,877 participants) found that long-term differences between surgical and conservative outcomes are much smaller than patients might expect – reoperation rates and long-term disability scores did not show significant differences.3
“Does home self-care really work?”
Yes. A 2024 systematic review and meta-analysis (12 RCTs, 1,545 patients) showed that digital self-management techniques measurably reduce pain intensity and pain-related functional disability in adults with chronic low back pain.5 The home “you-can-do-it-yourself” approach is scientifically supported.
“Which combination is most effective?”
The largest 2022 meta-analysis (58 RCTs, 10,084 patients) found that individualized, multimodal exercise – especially when combined with cognitive-behavioral elements – yields significant pain and functional improvements in chronic low back pain, with about a 38% added benefit compared to other active treatments.7 The message is simple: combining methods (exercise + EMS + softlaser + lifestyle changes) consistently provides better results than single modalities.
“What do international professional bodies recommend?”
The American College of Physicians (ACP) 2017 guideline lists exercise, softlaser, acupuncture, yoga, tai chi and massage among first-line non-drug treatments for chronic low back pain. Surgical intervention is recommended only if conservative care fails after 6–12 weeks.4 A 2024 international expert consensus (22 experts) specifically recommends softlaser and physiotherapy even for acute low back pain.
The gist
Top professional bodies and meta-analyses consistently support that for the vast majority of disc herniations and chronic low back pain, conservative, multimodal, home-performable treatment is the first choice. Along with exercise, EMS, softlaser, TENS and MENS can be integrated. This pillar article helps you choose among them.
Frequently Asked Questions
International guidelines (including the ACP 2017) state that the first-line treatment for disc herniation is conservative (non-surgical), and studies indicate many patients can avoid or delay surgery with timely home-based care and active rehabilitation. Surgery becomes necessary if there is clear neural injury (paralysis, sensory loss, urinary/fecal dysfunction) or if 6–12 weeks of conservative care yields no improvement.2, 4
Research evidence supports a multimodal approach. A typical home combination: regular exercise (base) + EMS (muscle strengthening) + softlaser (inflammation reduction) + TENS (for acute pain episodes). You don’t have to do everything at once – start with 1–2 methods and add more if needed.
TENS provides the fastest (within minutes) pain relief. Its effects last during the session and for hours after. Softlaser is cumulative – meaningful improvement after 10–14 days. EMS is the engine of longer-term (weeks–months) recovery. The three are complementary, each with different speed and depth.
At entry level a good-quality 4-channel stimulator and an entry softlaser start around 50,000–100,000 HUF. A complete home rehab package (EMS + softlaser + foam-roller) typically costs between 200,000–500,000 HUF. Compared to weekly private physiotherapy sessions, the investment can pay off within 6–12 months.
The three most important things: (1) regular movement (at least 3–4× weekly, 20–30 minutes), (2) strong core and spinal-supporting muscles (exercise + EMS if needed), and (3) correct posture (ergonomic chair, monitor height, proper lifting technique). The “don’t let it progress to a hernia” principle is the cheapest spine strategy.
The most common starter combination: a 4-channel muscle stimulator (e.g. Globus Premium 400 or Genesy 300 Pro) for muscle strengthening + an entry-level TENS function for pain relief (usually the same device provides both). With these two you can already make a big difference in most cases. Introduce softlaser later if inflammation reduction is a separate goal.
 Summary – Quick overview
Summary – Quick overview
References
- Wu A, March L, Zheng X, Huang J, Wang X, et al. (2020). Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Annals of Translational Medicine 8(6):299. PubMed: 32355743
- Penchev P, Ilyov IG, Todorov T, Petrov P-P, Traykov P. (2024). Comprehensive Analysis of Treatment Approaches for Lumbar Disc Herniation: A Systematic Review. Cureus 16(8):e67899. PubMed: 39328604
- Rickers KW, Pedersen PH, Tvedebrink T, Eiskjær SP. (2021). Comparison of interventions for lumbar disc herniation: a systematic review with network meta-analysis. The Spine Journal 21(10):1750-1762. PubMed: 33667683
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. (2017). Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Annals of Internal Medicine 166(7):514-530. PubMed: 28192789
- Scholz C, Schmigalle P, Plessen CY, Liegl G, Vajkoczy P, et al. (2024). The effect of self-management techniques on relevant outcomes in chronic low back pain: A systematic review and meta-analysis. European Journal of Pain 28(4):532-550. PubMed: 38071425
- Johnson MI, Paley CA, Jones G, Mulvey MR, Wittkopf PG. (2022). Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults: a systematic review and meta-analysis of 381 studies (the meta-TENS study). BMJ Open 12(2):e051073. PubMed: 35144946
- Fleckenstein J, Floessel P, Engel T, Krempel L, Stoll J, et al. (2022). Individualized Exercise in Chronic Non-Specific Low Back Pain: A Systematic Review with Meta-Analysis on the Effects of Exercise Alone or in Combination with Psychological Interventions on Pain and Disability. The Journal of Pain 23(11):1856-1873. PubMed: 35914641
