

 What is a leg ulcer?
What is a leg ulcer?
An ulcer is the death of the skin and underlying tissues, producing an open wound. A leg ulcer typically develops in the area between the ankle and the knee and is notoriously slow to heal. While a normal cut scars over in a few weeks, an ulcer can remain open for months or even years.
The reason is an underlying circulatory disorder: the tissues do not receive enough oxygen and nutrients, waste products are not removed adequately — so the wound becomes "stuck" in a chronic, non-healing state.
 Key point
Key point
The key to healing a venous leg ulcer (CEAP C6) is to support venous return. Regular activation of the calf muscle pump — by ACTIVE movement OR by a muscle stimulator, alongside compression therapy — can favorably affect wound healing. EMS is especially valuable when the patient is physically limited in movement. Another home modality is low-level laser therapy — the two can be combined.
Types of leg ulcers
According to origin, ulcers are classified into three main types:
| Type | Proportion | Background | Location |
|---|---|---|---|
| Venous | 70–80% | Varicose vein disease, venous valve insufficiency | Inner side of the ankle, shallow, irregular edges |
| Arterial | ~15% | Arterial narrowing, peripheral arterial disease | Toes, heel, anterior surface of the lower leg, deep, sharp edges |
| Diabetic | ~10% | Diabetes (neuropathy + microangiopathy) | Soles, toes |
This article focuses primarily on home muscle-stimulator support for the most common venous leg ulcer. In diabetic and arterial ulcers, treating the underlying disease takes priority — seek medical guidance.
 How does wound healing occur?
How does wound healing occur?
When you accidentally cut your finger, the wound may close within 2–3 days and a week later there is barely any trace. The body has a fantastic "self-healing" capacity. The injury sends a signal to the defence system: first, the clotting mechanism acts and seals the severed vessels. The bleeding stops.
After that, blood flow increases in the injured area. It brings many white blood cells that destroy pathogens and foreign material that entered the wound. Fresh blood is rich in oxygen and nutrients — these are needed to form the materials that close the wound. Healthy blood circulation is a prerequisite for wound closure.
 Analogy
Analogy
Imagine the whole process like a storm toppling an old tree in your garden. Normally you chop the branches and trunk, pile up the pieces, then fill the remaining hole with soil, level it and sow grass. In a few days there will be no sign of the hole left by the fallen tree. But if you don’t have tools to cut it up, don’t have the strength to carry it away, have nothing to fill the hole with and can’t get grass seed, the tree and the hole will mar the look of your garden for a long time. If a friend brings tools and helps, order is restored much faster.
A leg ulcer is similar: if your venous or arterial circulation is diseased, the poor circulation is precisely why the wound heals slowly. That is why you need to "call for help" to support blood flow.
Did you know what makes your blood circulate?
On many medical pages you can read about every drug, dressing and surgery — but the most fundamental information is often omitted or its importance not explained.
Your blood circulates continuously throughout your life. Your heart pumps it into the arteries, reaching every cell in your body. Your veins and lymphatic vessels collect it back, but it is the pumping action of your muscles that returns it to your heart.
Some of your muscle fibres (10–15%) are constantly contracted. Even if you don’t feel it, this muscle tone pumps your blood, even during sleep.
When you get up and start moving, that baseline is not enough. More blood flows into your limbs, and in the upright position it is harder to return it to your heart. That is why you need movement.
During everyday activities your muscles contract and squeeze blood out of the veins — just like squeezing toothpaste from a tube. When the muscle relaxes, the veins refill. Valves in veins and lymphatics allow flow only back toward the heart.
Little exercise = poor circulation
From the above you can see that if you do not move your muscles thoroughly and regularly, you create the conditions for poor circulation — and thus for ulcer formation.
Sitting at your desk all day or in the armchair in front of the TV voluntarily harms your circulation.
The most effective way to prevent ulcers (and many other diseases) is regular exercise. You do not have to be an athlete! Take a 30–40 minute walk in the evening around your neighbourhood. Hike, do Nordic walking, jog, cycle, swim, practise yoga, do calisthenics, dance. It doesn’t matter which. The point is to move your muscles thoroughly every day.
This will "boost" your circulation. You can prevent ulcers, symptoms of peripheral artery disease and many other problems.
What can you do to help a leg ulcer heal?
If you failed to prevent it and an ulcer has developed, things are already more difficult. Move as much as you can without pain.
If you can no longer manage to move, use a modern medical device: replace muscle movement with a functional electrical stimulator (FES) or muscle stimulator (EMS). With this treatment your muscles contract rhythmically; the effect is similar to walking or strolling. It supports venous blood flow and can favourably influence the healing chances of a leg ulcer.
 Important warning
Important warning
If you have a pacemaker or an implanted defibrillator, DO NOT use electrical treatment. It is also contraindicated when active thrombosis is suspected — see the detailed contraindication list in section 9.
Leg ulcer treatment with electrotherapy – protocol
The treatment is very easy to perform. Stick the stimulator device electrodes onto the calf muscles, select the treatment program, then set the intensity so that you feel definite but not painful muscle contractions.
Treatment basic parameters
- Duration: 20–30 minutes daily, possibly repeated twice.
- Electrode placement: along the midline of the calf musculature (follow the device manual). Do not place electrodes directly on the wound.
- Current intensity: perceptible, rhythmic contractions — definite but not painful.
- Course: continue until full wound closure (often 2–4 months, longer in more severe cases).
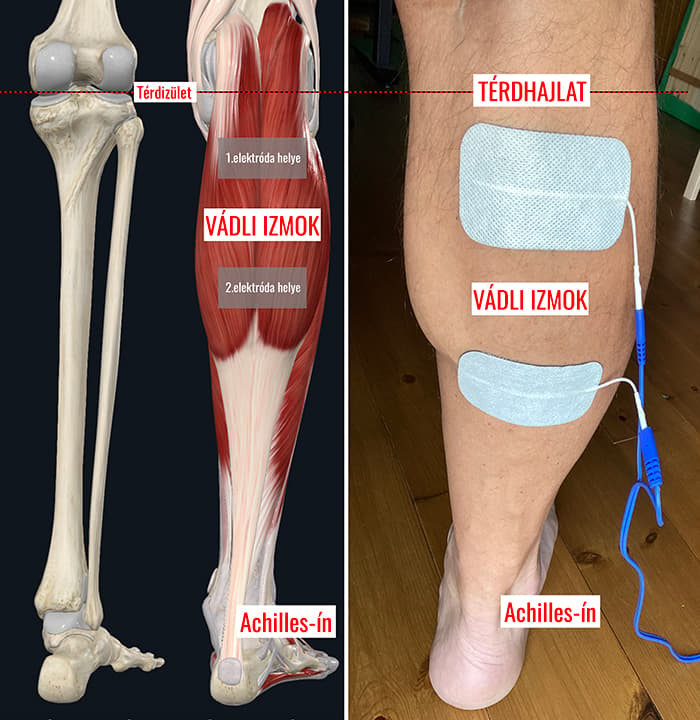
Electrode placement
I prepared a diagram showing where to stick the electrodes. Place the electrodes on the calf muscles — not directly on the ulcer. Two electrodes typically lie on the upper calf and two on the lower third of the calf, along the midline.
What to expect?
The more severe the condition, the more often you need to exercise your muscles thoroughly. You can treat even large ulcers — it is important not to place electrodes directly on the wound.
During the first treatments your pain may temporarily increase. This is because the accelerated blood flow begins to wash out accumulated toxins from the ulcer (decomposition products from cell death), which causes pain. Don’t worry — this is a sign that the healing process has started. After a few days the pain will subside.
Healing takes time — it does not happen in minutes or even days. But if you support circulation, it will repay you with healing.
 Home devices – muscle stimulator devices
Home devices – muscle stimulator devices
Elite SII TENS/EMS device
Multifunctional 2-channel device with 100 programs: EMS and pain-relieving TENS functions. An ideal choice to support leg ulcer care, as it can also be used to relieve pain around the wound.
Rehalito EMS muscle stimulator
Simple, affordable 2-channel device. Specifically designed for rehabilitation and circulation support.
Myolito TENS/EMS/FES device
Multifunctional electrotherapy device with TENS, EMS and FES programs — functional electrical stimulation to target the calf muscle pump.
 Before you start treatment – contraindications
Before you start treatment – contraindications
For safe use, know the contraindications.
When NOT to use a muscle stimulator?
- Implanted cardiac pacemaker or defibrillator
- Suspected acute thrombosis or recently diagnosed DVT
- Active purulent skin infection in the treatment area
- Malignant tumour in the treatment area
- Pregnancy (abdomen and lumbar region)
- Severe arterial insufficiency (critical limb ischemia) – medical consultation required
Important note
Before starting treatment for a leg ulcer always consult your treating physician: active thrombosis suspicion and possible arterial ischemia must be excluded. Read the device user manual.
Other home modalities alongside ulcer treatment
The muscle stimulator is not the exclusive solution — successful leg ulcer treatment is teamwork and composed of a combination of modalities:
- Medical supervision – diagnosis and treatment of the underlying disease.
- Compression therapy – the most important pillar for venous ulcers (compression stockings or bandaging, fitted by a professional).
- Appropriate wound dressing – ensuring a moist wound-healing environment.
- Movement – activating the muscle pump supports venous return.
- Muscle stimulator (EMS/FES) – the main topic of this article.
- Low-level laser therapy (photobiomodulation) – a parallel home modality, combinable with EMS.
- Lymphatic massage device (pneumatic compression) – to support venous return in more severe venous circulation disorders.
 My advice – how to combine?
My advice – how to combine?
Compression stockings and daily regular movement (or a muscle stimulator if you cannot move) are the foundation. With physician approval you can add low-level laser therapy and pneumatic compression on top. Modalities do not exclude each other; they support each other.
When NOT to expect miracles?
Start with realistic expectations. A muscle stimulator will not heal an ulcer if:
- You do not treat the underlying disease – in venous insufficiency wearing compression stockings is essential; in diabetes glycaemic control is indispensable.
- Severe arterial insufficiency is present – if blood supply is critically low, this must be addressed first (possibly with vascular surgery).
- The wound is infected – with active purulent infection, antibiotic treatment is required first.
- You do not follow hygiene rules – without regular dressing changes and wound cleaning, the stimulator will not help.
EMS is a valuable adjunct — but it does not replace medical care and treatment of the underlying disease.
 Scientific background
Scientific background
Electrical stimulation in healing venous leg ulcers
Houghton and colleagues (2010) showed in a randomized clinical trial that electrical stimulation combined with conventional wound care can favorably influence the healing rate of venous leg ulcers.1
Compression therapy in venous leg ulcers
Robertson and colleagues' Cochrane review (2014) considers compression therapy the cornerstone of venous leg ulcer management — without compression the wound-healing rate is significantly reduced and recurrence increases.2
Calf muscle pump and venous return
Padberg and colleagues (2004) demonstrated in a randomized trial that structured exercise provides significant improvement in calf muscle pump function over 6 months in chronic venous insufficiency — the basis for replacing it with muscle stimulation.3
ESVS 2022 European clinical guidelines
De Maeseneer and colleagues edited the European Society for Vascular Surgery 2022 Clinical Practice Guidelines on the management of chronic venous disease, which include treatment algorithms for CEAP C5–C6 stages.4
Frequently asked questions
Healing of a venous leg ulcer is always lengthy: optimally 8–16 weeks, and in more severe cases several months. EMS complements conventional treatment (compression, wound dressing, treatment of underlying disease) and can favourably influence the healing process. Continue treatment until complete wound closure.
Yes, the two modalities work via different mechanisms: EMS supports venous return by activating the muscle pump, while low-level laser promotes cellular regeneration. They can be combined with physician approval — a detailed laser protocol is available in the parallel article.
On the midline of the calf muscles — avoiding the ulcer. Electrodes MUST NOT be placed directly on the open wound or its immediate vicinity. The device manual contains precise placement instructions, and your treating physician can advise you.
During the first days to weeks a temporary increase in pain at the ulcer site may occur as accelerated circulation flushes out accumulated toxins. This subsides after a few days and is a sign that healing has started. If pain is severe or persistent, stop treatment and consult your physician.
In the case of active purulent infection (erysipelas, cellulitis) suspend EMS treatment and seek immediate medical attention: antibiotic therapy is required. Details on infectious complications: erysipelas – bacterial skin infection.
 Summary – quick overview
Summary – quick overview
Sources
- Houghton PE et al. (2010). Electrical stimulation therapy increases rate of healing of pressure ulcers in community-dwelling people with spinal cord injury. Arch Phys Med Rehabil. PubMed: 20382279
- Robertson L et al. (2014). Compression for venous leg ulcers. Cochrane Database Syst Rev. PubMed: 25387769
- Padberg FT Jr, Johnston MV, Sisto SA (2004). Structured exercise improves calf muscle pump function in chronic venous insufficiency: a randomized trial. J Vasc Surg. PubMed: 14718821
- De Maeseneer MG et al. (2022). European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs. Eur J Vasc Endovasc Surg. PubMed: 35027279
