PeroBravo for the treatment of peripheral paralysis
PeroBravo is a versatile stimulator device with 20 different programs that the patient can use at home without the presence of a physician. Its main application area is the treatment of peripheral paralysis of varying severity. Thanks to a special foot sensor it is suitable for treating peroneal nerve palsy and the resulting gait disorder (foot drop).
Why is electrical treatment needed in paralysis?
Peripheral paralysis is caused by injury or dysfunction of the so-called "lower motor neuron", i.e. the motor nerve running from the spinal cord to the muscle. It can arise for various reasons and can be of different degrees of severity.
Because the nerve fiber does not function, the brain's impulse does not reach the affected muscles, so there is no muscle contraction and no movement can occur.
A muscle that has lost its motor nerve is referred to in medical practice as a "denervated muscle".
After the loss of nerve connection (denervation), the muscle goes through three stages:
- immediate loss of voluntary motor function
- rapid decrease in muscle mass (muscle atrophy) and loss of muscle structures (sarcomeres), and
- degeneration of muscle fibers, during which connective tissue and fat replace the muscle fibers. This is a permanent condition.
Regular electrotherapy slows down or completely prevents the atrophy process, so the muscle's functionality can be maintained until the nerve regenerates.
Nerve healing and regeneration is a very slow process. A nerve fiber typically regenerates at about 0.1–0.2 mm per day, and even in the most favorable cases not more than about 1 mm per day. In the case of a lumbar nerve injury, the nerve length to the toes can be 60–80 cm. That means it can take years until the nerve once again "reaches the muscle", i.e. until regeneration is complete.
The muscle cannot survive that long without its nerve. Without contractions the muscle will degenerate within one and a half to two years: connective tissue replaces muscle tissue, and even if the nerve regenerates, the muscle may already be nonfunctional and the paralysis will remain.
Therefore, during the long recovery of paralysis it is most important to maintain the muscle in a functional state, even though for 1–2 years there may be no visible "result". This is what the PeroBravo is for.
Peripheral paralysis requires special impulses
You must prevent muscle atrophy until the nerve regenerates. Repeated stimulation pulses also accelerate nerve regeneration.
Treatment of a paralyzed muscle varies depending on the degree of denervation. The PeroBravo can be used for all forms.
While a healthy muscle can be made to contract with short-duration rectangular pulses, a denervated muscle does not respond to these. In such cases the muscle is treated with long, slowly rising triangular pulses of up to 600–800 milliseconds. Partially denervated muscles can be treated with triangular or trapezoid-shaped pulses.
Contractions are elicited by pulses with a long rise. This activates the paralyzed muscle while at the same time preventing contraction of surrounding healthy muscles.
With partial denervation and as therapy progresses successfully, the pulses can be progressively shortened (600–400–200 ms), and trapezoids can replace the triangles. Only such adjustments should be made that the partially denervated muscle still responds to the stimulus.
Optimal treatment parameters can be determined individually. The device supports recording the intensity/duration curve.
Peroneal nerve palsy
One of the most common peripheral paralyses (pareses) is peroneal (fibular) nerve palsy.
In the initial stages of treating peroneal palsy you should use triangular, then trapezoid pulses as described above. When the nerve fiber again reaches the muscle, the muscle will be ready to accept rectangular pulses and you can begin muscle strengthening.
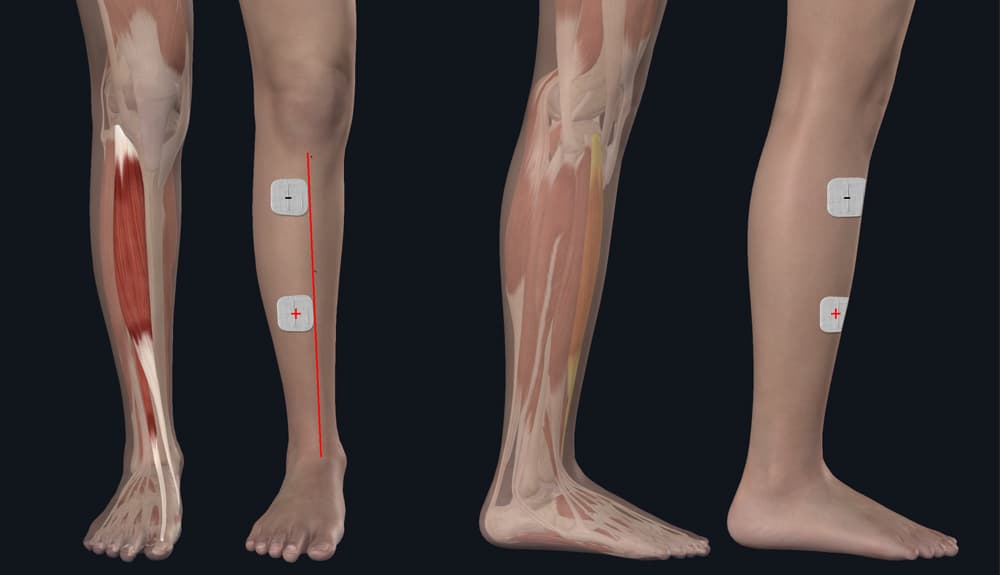
In the illustration I show which muscle is involved. Peroneal palsy affects the muscles on the anterolateral side of the shin (mainly the tibialis anterior). These muscles lift the foot, i.e. enable dorsiflexion at the ankle. If they do not work, you cannot lift your foot and toes upward (dorsiflexion). During walking a "dropped" foot hinders the step. Your gait becomes characteristically waddling and unsteady.
To determine electrode placement, palpate along the edge of your shinbone (marked by a red line in the picture). Place the first electrode about 5–8 cm below your kneecap over the muscle. The inner edge of the electrode should touch the shin edge and the electrode should extend outward from there. Connect the negative pole of the cable to this electrode.
Place the other electrode lower on the muscle, roughly at the mid-shin level or slightly below. Connect the positive pole to this electrode.
If you use a rubber electrode and sponge instead of a self-adhesive electrode, the picture shows the latter: a wet sponge in a cover fixed in place with an elastic strap.
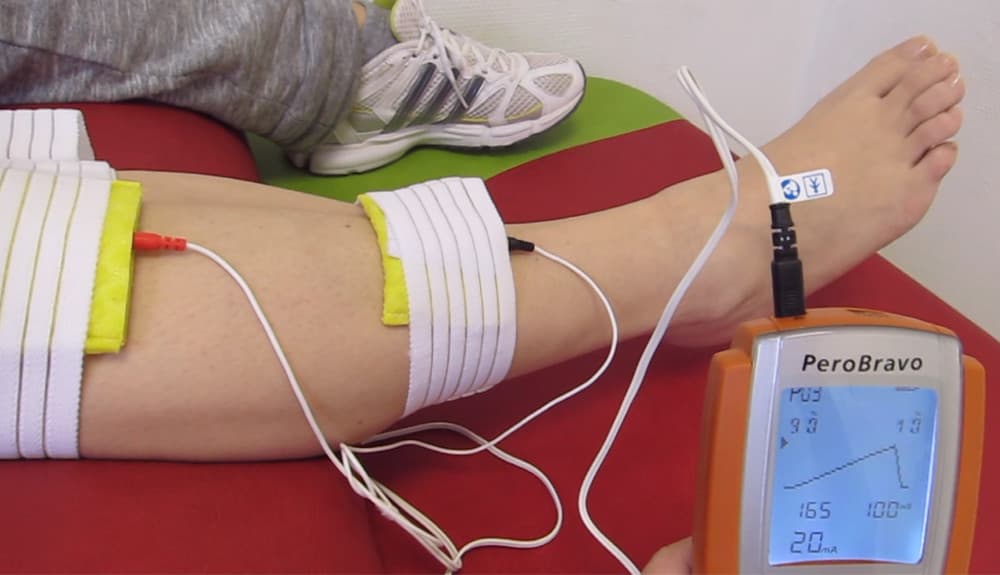
The next phase is retraining gait. For this use the PeroBravo's special accessory, the foot sensor. It senses when your heel touches the ground. This activates the device, which then delivers an assisting impulse to the peroneal muscle to help lift the foot.
Because relearning a movement requires about 10,000 repetitions by the brain, this phase also requires persistent treatment and training.
Facial nerve paralysis (Bell's palsy)
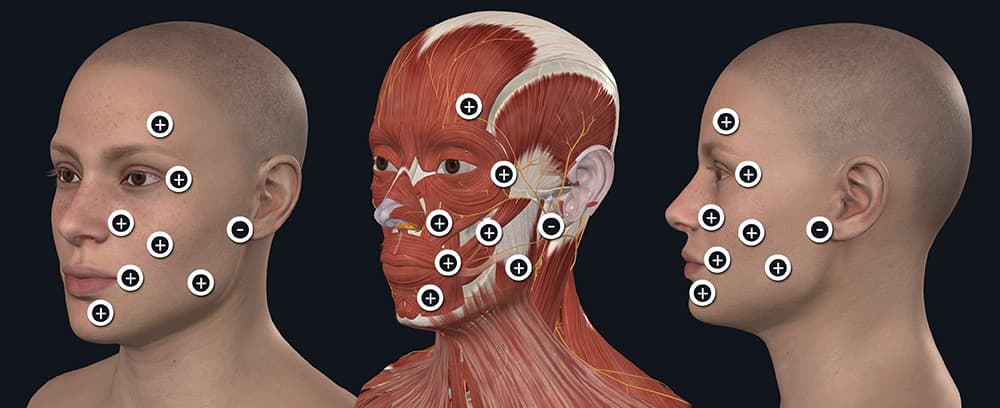
Another common peripheral paralysis (paresis) affects the facial nerve. This paralysis is also called Bell's palsy. Its consequence is that the facial mimic muscles do not work (you cannot wrinkle your forehead, close your eye, the corner of your mouth droops and saliva may run out, etc.). Because it is usually one-sided, the face becomes asymmetric. The muscles on the healthy side pull the affected side toward them.
Treatment here also depends on the degree of nerve fiber damage. In complete damage the treatment starts with triangular pulses, then as the condition improves progressively shorter pulses are used, then trapezoid pulses, and finally rectangular waves. In complete paralysis it can take more than a year to return to a near-normal state. Complete (100%) recovery requires exceptional luck; usually some degree of residual difference remains.
For this treatment you will need small-diameter (about 25–30 mm), round self-adhesive electrodes (you can get these here). The face has little space, so large electrodes simply won't fit and you cannot treat precisely enough with them.
PeroBravo – rehabilitation in a single device
With the PeroBravo device you have a therapeutic option that provides solutions for all degrees of peripheral paralysis.
The initial treatment of severe paralysis is covered by programs 1–6, 17, 18, while improving paresis is addressed by programs 7–11, 19, 20.
A special diagnostic program (PRG 12) allows determination of the intensity/duration curve. This is intended so that the most appropriate treatment parameters for you can be accurately defined.
You can use the foot sensor with programs 13–16; these help synchronized gait retraining in peroneal palsy.
The device can be used not only for denervated muscle treatment. Programs 10, 19, 20 can also be applied for rehabilitation of muscles with intact innervation or for pain relief.
Program structure
The device's programs were designed to accompany the patient from severe peripheral nerve injury to full recovery. This progression is reflected in programs 1 to 10, where program 1 is for complete nerve injury, while program 10 is for a muscle with a healthy motor nerve.
In complete nerve injury you must start with program 1. A muscle that has completely lost its motor nerve can only be brought to contraction by a very long impulse, nearly 1 second in duration. Moreover, the impulse must rise slowly and gradually. Therefore the duration of the rising phase (in percentage) can be set. Initially the rising phase constitutes 90% of the pulse duration. Since regeneration from complete paralysis can take years, program 1 should be used initially with a 90%–10% rise/fall ratio, then the rise time can be gradually shortened as you monitor results.
Over time you should check whether the shorter-duration program 2 can elicit an adequate contraction. If yes, switch to program 2, then to program 3. Progress step by step, possibly until full recovery.
From the above it follows that since not everyone has a complete nerve injury but rather some degree of partial injury, program 1 may not be appropriate for partial injuries. It is too long and a partially damaged nerve signals it as an unpleasant "shock." You must find the program that produces a good contraction but is not unpleasant.
There are two methods for this. One is to try the programs in sequence (don't worry — none of them can harm you, at worst you'll notice it's not the right one). After a few minutes of trying you will find the suitable one. The other method is provided by the device itself for physiotherapists: program 12, which in 24 steps helps determine the most appropriate intensity/duration. This is usually performed by clinic professionals. If you do not receive help from a physiotherapist, the first method will yield the same result.
Creating individual programs
The device allows you to create a personalized program in program slots 19 and 20 according to your treatment needs, which can consist of up to 5 different phases.
This way you can optimize the PeroBravo for treating a range of conditions:
Muscle stimulation
- Improvement of blood flow and circulation
- Relief of muscle spasticity (stiffness)
- Muscle strengthening
- Avoiding imbalances developing within the muscle
- Activation of muscle fibers
- Muscle fatigue
- Strengthening of wasting muscles
- Muscle regeneration
- Preservation and expansion of mobility
Nerve stimulation (pain therapy)
- Stimulation of endorphin production
- General pain relief and pain therapy, including for:
- Arthritis
- Back pain
- chronic back pain
- cervical spine pain
- thoracic spine pain
- lumbar spine pain
- Circulatory problems
- Nerve pain
- Muscle pain
- Phantom pain
- Pain after bone fracture
- Pelvic floor pain