
 What is thrombosis?
What is thrombosis?
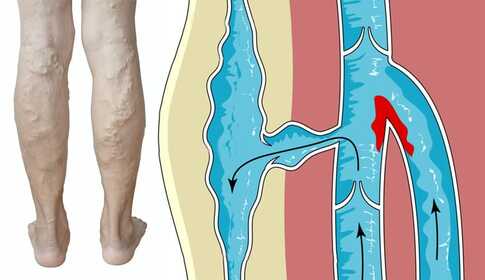
Thrombosis is the "clotting" of blood inside a vessel: a blood clot (medically called a thrombus) forms and, like a plug, partially or completely blocks the vein. Blood cannot flow freely toward the heart, resulting in increasing, tense pain and swelling in the affected area.
Thrombosis most commonly develops in the leg, especially the lower leg – depending on which venous system is affected we distinguish two basic forms: superficial and deep vein thrombosis. The clinical significance of these two forms is fundamentally different.
 Key point
Key point
Thrombosis is not a single disease entity: superficial thrombosis is milder and often manageable on an outpatient basis; deep vein thrombosis (DVT), by contrast, can be life-threatening because it may lead to pulmonary embolism. Acute DVT requires hospital treatment – at home you can only perform prevention and post-thrombotic aftercare.
 How does it develop? – Venous circulation and Virchow's triad
How does it develop? – Venous circulation and Virchow's triad
Basics of venous circulation
Veins run throughout your body. They collect used blood and return it to your heart, then to the lungs to receive fresh oxygen; the arteries deliver oxygenated blood back to your organs. Superficial veins collect blood from the skin, mucous membranes and areas close to the body surface – they do not run directly back to the heart at the surface but join the larger deep veins that run between the tissues. These large "channels" lead to the heart.
Blood flows in the veins passively. During movement your muscles contract, compress the veins and squeeze blood out of them. Blood always moves toward the heart because the valves in the veins act as gates allowing flow only in that direction. This so-called muscle pump is the natural engine of venous circulation.
If you move little, the muscle pump does not work: blood pools, flows slowly and the tendency to clot increases. This is one central mechanism in thrombosis formation.
Virchow's triad – three factors that together lead to thrombosis
Classically three factors are distinguished in the development of thrombosis (Virchow, since 1856, forms the basis of vascular medicine):
- Injury to the vessel wall (e.g. venous injury, inflammation, vascular catheter).
- Changes or slowing of blood flow (lack of movement, prolonged sitting/lying, severe varicose vein disease).
- Changes in blood composition, increased coagulability (inherited clotting disorders, hormonal factors, malignant disease, smoking).
Each factor alone poses a risk; when present together the probability of thrombosis increases multiple times.
Types of thrombosis – superficial vs. deep vein
| Characteristic | Superficial thrombosis | Deep vein thrombosis (DVT) |
|---|---|---|
| Where does it develop? | Veins close to the skin surface | Deep veins running between muscles |
| Severity | Milder, often manageable on an outpatient basis | Can be life-threatening – risk of pulmonary embolism |
| Typical symptom | Local redness, tender nodule/induration along the vein | Unilateral leg/lower-leg swelling, pain, warmth |
| Urgency | Medical consultation, usually outpatient | URGENT – hospital treatment required |
| Risk of pulmonary embolism | Low | High |
Superficial thrombosis (phlebitis)
Thrombosis that develops in veins close to the skin surface, often in tortuous, dilated varicose veins. A stripe-like redness along the vein and a tender, sometimes firmer lump can be felt. The condition usually resolves on its own or can be treated on an outpatient basis – nevertheless always consult a doctor, because rarely it can extend to the deep venous system.
Deep vein thrombosis (DVT) – the “sneaky enemy”
Estimatedly 16–20 thousand people in Hungary develop DVT each year, and many die from its complications. It is called the “sneaky enemy” because it often appears suddenly without marked warning signs – and due to the risk of pulmonary embolism it can immediately become life-threatening.
The thrombus that forms in a deep vein adheres to the vein wall and grows. If a fragment breaks off, the bloodstream carries it to the heart and then to the lungs – this is pulmonary embolism. Depending on its size, the clot blocks one of the lung arteries: occlusion of a larger pulmonary artery often causes immediate death; a smaller embolus leads to infarction of the affected lung tissue (pulmonary infarction) and always heals with consequences.
Symptoms and warning signs of thrombosis
Thrombosis often develops insidiously and unnoticed. In most cases there are no obvious early warning signs. The disease usually begins with:
- swelling of your ankle, foot or lower leg;
- severe, tense pain in the affected area;
- the skin becomes red and the swollen area feels warm.
The classic, “textbook” DVT symptom triad is sudden-onset unilateral limb swelling, pain and redness – but in a significant portion of patients the symptoms are more subtle or nonspecific.
 When should you call an ambulance immediately (dial:112)?
When should you call an ambulance immediately (dial:112)?
The following symptoms may indicate pulmonary embolism – do not wait, call emergency services:
- sudden chest pain, shortness of breath, rapid breathing;
- sudden onset cough, possibly with blood-streaked sputum;
- rapid heartbeat, dizziness, fainting;
- sudden unilateral leg swelling within half a day plus any of the above symptoms.
What increases the risk of thrombosis? Risk factors
Many predisposing factors are known. The risk is higher when several factors are present together.
- Prolonged immobility – “forced rest”, postoperative hospital stay, casting after a fracture. Muscles do not pump venous blood, flow slows and blood may clot.
- Prolonged sitting – hours in a car, a long flight (see travel-related thrombosis).
- Venous injury or surgery – may increase the risk of clot formation; veins dilate under general anesthesia.
- Certain cancers – can increase levels of substances that promote clotting, and a growing tumor can compress surrounding veins.
- Inherited clotting disorder (e.g. Leiden mutation, antithrombin deficiency).
- Heart failure – weakened heart slows blood flow.
- Pacer, central venous catheter – can irritate the vessel wall and slow blood flow.
- Contraceptive pills, hormone therapy – can increase blood coagulability.
- Smoking – greatly affects clotting and circulation.
- Pregnancy – the growing fetus can compress pelvic and leg veins, slowing circulation. See the special situation in the pregnancy varicose veins article.
- Severe obesity – adversely affects venous circulation.
- Varicose vein disease – venous stasis increases risk. Details in the chronic venous insufficiency article.
- Previous thrombosis – those with prior DVT or pulmonary embolism have a higher chance of recurrence.
Special situation: travel-related thrombosis
One feared complication of long travel is deep vein thrombosis. Blood circulation slows in a limb immobilized for many hours and pooled blood can clot in the vessels. When you then stand up, contracting muscles may dislodge the clot – it can travel to the heart and then the lungs, causing life-threatening pulmonary embolism.
In addition to forced immobility, other predisposing factors may play a role: tortuous, dilated varicose veins, increased blood coagulability, use of contraceptives and hormone preparations, vessel wall disease, smoking, overweight and an already sedentary lifestyle. If these affect you, you belong to a higher-risk group – not a reason to panic, but to prepare.
Prevention on long trips
- Hydration: drink plenty of fluids, avoid alcohol and excessive caffeine.
- Compression stockings: 15–20 mmHg preventive stockings for long flights and car trips.
- Move hourly: if driving, stop at rest areas and walk around a few times; on flights get up and walk in the cabin.
- In-seat exercises: while seated, perform heel raises and foot dorsiflexion 20–30 times to engage the calf muscle pump.
- Home device: if you have predisposing factors, consider carrying a portable muscle stimulator.
 My tip for long journeys
My tip for long journeys
The most important measure is to interrupt sitting and regularly activate the calf muscle pump. Even 5 minutes of walking every 1–2 hours significantly reduces venous blood stasis. Compression stockings and ample fluid intake are always recommended on long trips.
What to do if you suspect thrombosis
If you notice any of the symptoms above, seek medical attention immediately – with as little movement as possible. Once the thrombosis process has started, there is little you can effectively do at home; delaying will only worsen the situation.
 Important to know
Important to know
Treatment of fresh, acute deep vein thrombosis can take place only in hospital, where specialists provide anticoagulant and circulation-supporting medications and, if needed, catheter interventions. Home therapeutic devices are forbidden in the acute phase.
If thrombosis is suspected while you are at home or on the road, do not perform leg exercises as movement may dislodge the clot. Rest and get medical evaluation as soon as possible.
Acute complication: pulmonary embolism
The most feared complication of DVT is pulmonary embolism. Fortunately it develops only in some cases – but when it occurs it represents acute life-threatening danger.
If the entire clot formed in the vein moves from its place or a fragment breaks off, it is carried by the bloodstream to the heart and then to the lungs – this is embolization. A clot that reaches the lungs is called a pulmonary embolus. Depending on its size, the clot blocks one of the lung arteries, creating a sudden, severe condition:
- occlusion of a larger pulmonary artery often causes immediate death;
- a smaller embolus leads to infarction of the affected lung area (pulmonary infarction) and inevitably heals with sequelae.
Pulmonary embolism – call emergency services immediately (dial: 112)!
- sudden chest pain, palpitating heartbeat;
- shortness of breath, air hunger, rapid-shallow breathing;
- cough, possibly with blood-streaked sputum;
- dizziness, fainting, pallor, cold sweat.
Any of these symptoms occurring together with sudden unilateral leg swelling is highly suspicious – the patient should not move; call an ambulance immediately.
 Late complication: post-thrombotic syndrome (PTS)
Late complication: post-thrombotic syndrome (PTS)
After a thrombosis you will never be exactly as before. The disease always ends with a “residual condition” that you will live with for the rest of your life. This is the post-thrombotic condition – medically called post-thrombotic syndrome (PTS).
The clot continuously changes: part of it is absorbed, part is replaced by scar tissue. By 90–120 days after thrombosis the process becomes definitive. Circulation in the affected leg will not be the same as before – the vein wall and venous valves are permanently damaged and venous return remains chronically impaired.
How many symptoms remain depends on many factors: size of the thrombus, speed of treatment, individual coagulation and regenerative characteristics. About 20–50% of patients develop mild-to-moderate PTS, and 5–10% develop severe forms – even with appropriate anticoagulant therapy.
Typical symptoms of PTS
- persistent swelling of the affected limb;
- tense pain, “heavy leg” sensation;
- brownish-purple-reddish skin discoloration (hemosiderin deposition) – see Red-brown spot on the lower leg – what is it?;
- dry, cracked skin, yellowish discharge (lymph) leakage;
- in severe cases chronic, slowly or non-healing venous leg ulcer.
Goals of home treatment
- prevent recurrence of thrombosis;
- reduce symptoms of the residual condition;
- avoid severe complications (venous leg ulcer).
Regular exercise – the cornerstone of PTS management
The natural motor of venous circulation is the calf muscle pump. If you have had thrombosis and are physically able, regular exercise is your most important tool. Never stop.
I do not mean competitive sport: regular walking is perfectly appropriate. If your condition only allows you to walk a few circuits of the room, do that – but do it several times a day. If you can, jog or cycle at least 3–4 times a week for at least one hour each time (more is better).
Home devices – when active movement is limited
If paralysis, muscle weakness, significant overweight, joint pain, post-surgical state or long travel prevents sufficient movement, home medical devices can support the calf muscle pump effect.
Muscle stimulator (EMS) devices
EMS devices trigger rhythmic contractions of the calf muscles with electrical impulses – exactly mimicking what happens during walking. In PTS and as adjunct thrombosis prevention, daily 20–30 minute sessions can support venous circulation. Detailed selection and product range are on the category page.
Lymphatic massage device (pneumatic compression, IPC)
The air-chamber cuff inflates and deflates the chambers sequentially, thus "massaging" the leg from bottom to top. It is especially recommended in PTS because it supports both venous and lymphatic circulation – it has well-documented evidence in reducing chronic swelling and tense pain.
Power Q-1000 Plus lymphatic massage device
Entry-level home device for mild-to-moderate PTS symptoms.
Power Q-2200 lymphatic massage device
Mid-range device with multiple treatment programs – for pronounced, often recurrent swelling.
Power Q-1000 Premium lymphatic massage device
Advanced home device with multiple programs and greater comfort – for more severe PTS and chronic venous insufficiency.
How to prevent recurrence of thrombosis?
If you have already had a thrombosis, the risk of recurrence is significant – you must look after yourself for life. Thrombosis is much easier to prevent than to treat.
- Take the medications prescribed at hospital discharge regularly.
- For some "blood thinner" drugs, your blood's “coagulability” must be monitored regularly – the required dose may change according to current lab values. Newer (DOAC) agents usually do not require such close control.
- Never change medication doses on your own – only after consulting your treating physician.
- Attend regular lab check-ups (usually monthly to bimonthly) and discuss results with your doctor.
- Overanticoagulation can cause bleeding: spontaneous gum bleeding, prolonged bleeding after a needle stick, or unexpected bruising are warning signs.
- Move daily – 60–70 minutes of walking, jogging, cycling (possibly in several sessions). Do not underestimate the importance of activity.
- Do not embark on long car, bus or plane journeys without preventive measures – stand up and walk every half hour.
- If you smoke, quit.
- If you take contraceptives, discuss switching options with your doctor.
- If you are overweight, gradually lose a few kilos with diet change and regular exercise.
- Anticoagulant treatment after thrombosis is usually required for 3–6 months. The treating physician will decide whether to continue thereafter – if you do not reduce your risk factors, medication may be required lifelong.
 Home devices – when NOT to use them?
Home devices – when NOT to use them?
There are absolute contraindications to the use of home devices recommended for PTS (muscle stimulators, lymphatic massage devices) – know these for safe use.
When NOT to use a lymphatic massage device (IPC)?
- Acute deep vein thrombosis – hospital treatment required, home IPC is forbidden
- Suspected or confirmed acute pulmonary embolism
- Severe, decompensated heart failure
- Acute skin infection, eczema or open wound at the treatment area
- Active malignant tumor in the treatment area without treating physician's permission
When NOT to use a muscle stimulator (EMS)?
- Implanted pacemaker or defibrillator
- Suspected acute thrombosis or newly diagnosed DVT
- Infected or inflamed skin at the treatment area
- Malignant tumor in the treatment area
- Pregnancy (abdomen and lower back region)
Important to know
Before starting any home device, ask your treating physician – especially in PTS where the clinical picture and coagulation status vary individually. Read the device manual.
 Scientific background
Scientific background
Global burden of venous thromboembolism
According to the review by Heit and colleagues (2016), venous thromboembolism (DVT and pulmonary embolism combined) is one of the most common causes of death in hospitalized and outpatient populations; about 30% of patients experience recurrence within 10 years after the initial episode.1
Compression stockings on long flights
Clarke and colleagues' Cochrane review (2021) found that for asymptomatic, higher-risk passengers on flights longer than four hours, wearing graduated compression stockings significantly reduces the incidence of asymptomatic DVT and leg edema.2
Clinical management of post-thrombotic syndrome
The consensus by Kahn and colleagues (2021) states that in PTS clinical practice, graduated compression therapy and structured physical activity (calf muscle pump program) are the main pillars; intermittent pneumatic compression as an adjunct to compression stockings can further reduce symptoms.3
Pneumatic compression and venous return
In the clinical trial by Kakkos and colleagues (2001), intermittent pneumatic compression favorably influenced venous circulation and alleviated symptoms of chronic venous insufficiency – relevant for home treatment of PTS as well.4
ESVS 2022 European clinical guidelines
De Maeseneer and colleagues edited the European Society for Vascular Surgery (ESVS) 2022 clinical practice guidelines on the management of chronic venous disease and post-thrombotic syndrome, which set the current standard for treatment algorithms.5
Frequently asked questions
Superficial thrombosis develops in veins close to the skin, is usually treatable on an outpatient basis and has a low risk of pulmonary embolism. Deep vein thrombosis (DVT) affects the deep venous system, can be life-threatening and requires hospital treatment for anticoagulation and pulmonary embolism prevention.
Flights longer than four hours can increase DVT risk, especially if other risk factors are present (varicose veins, contraceptives, smoking, overweight). Prevention includes 15–20 mmHg compression stockings, ample fluid intake and getting up to move hourly – see details in the travel-related thrombosis section.
PTS is the most common late complication of DVT – it occurs in 20–50% of patients in mild-to-moderate form and in 5–10% in severe form. Symptoms include persistent leg/lower-leg swelling, heavy-leg sensation, brownish-purple skin discoloration (hemosiderin), and in severe cases venous leg ulcer. See the PTS section for details and home management.
Acute deep vein thrombosis can only be treated in hospital (anticoagulation, imaging, possibly catheter intervention). Home physiotherapy devices are FORBIDDEN in the acute phase. In the PTS phase (after hospital treatment), however, home exercise, compression stockings, muscle stimulators and pneumatic compression are important parts of long-term management.
Yes, with your treating physician's permission, pneumatic compression may be used at home as a key PTS treatment about 3–4 months after hospital acute care. It is FORBIDDEN in the acute phase and contraindicated with active DVT or suspected pulmonary embolism – see the detailed contraindication list in section 11.
After an acute DVT, anticoagulant therapy is generally required for 3–6 months. Whether to continue afterward is decided by the treating physician based on risk factors and recurrence probability. In severe or recurrent DVT, or when risk factors cannot be reduced, treatment may be lifelong.
 Summary – quick overview
Summary – quick overview
Sources
- Heit JA (2015). Epidemiology of venous thromboembolism. Nature Reviews Cardiology. PubMed: 26076949
- Clarke MJ et al. (2021). Compression stockings for preventing deep vein thrombosis in airline passengers. Cochrane Database of Systematic Reviews. PubMed: 34611891
- Kahn SR et al. (2021). The post-thrombotic syndrome: evidence-based prevention, diagnosis, and treatment strategies. Hematology American Society of Hematology Education Program. PubMed: 34889360
- Kakkos SK et al. (2001). Improved hemodynamic effectiveness of a new intermittent pneumatic compression system in patients with chronic venous insufficiency. Journal of Vascular Surgery. PubMed: 11700495
- De Maeseneer MG et al. (2022). European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs. European Journal of Vascular and Endovascular Surgery. PubMed: 35027279
