Facial nerve palsy and its treatment
The facial nerve (nervus facialis) is the seventh cranial nerve (VII) and performs several functions. It acts as a motor nerve for the facial mimic muscles and thus determines your facial expression. Its branch to the tongue is responsible for taste (the anterior one third of the tongue). It also contributes to tear and saliva production. Facial nerve palsy heals slowly and can take up to a year. Although the first 5–10 treatments are usually given in a clinic, that is not enough! You must continue electrotherapy at home until full recovery.
Facial nerve palsy is paralysis—usually unilateral—of certain facial muscles innervated by the facial nerve (n. facialis), especially the mimic muscles.
Of the twelve (XII) cranial nerves, the facial nerve is the seventh (VII). It is paired, which means there is one on the right and one on the left. Cranial nerves originate from nerve nuclei in the brain and run directly to their target organs (muscle, gland, etc.).
All other nerves supplying the periphery (arms, legs, trunk) travel indirectly: they synapse in the spinal cord and reach their targets from there.
The facial nerve supplies the mimic muscles (forehead, eye area, nose, mouth and one cutaneous neck muscle—the platysma), the stapedius muscle in the ear canal, parts of the pharyngeal musculature, the anterior two thirds of the tongue for taste (sensory), and virtually all glands in the head (visceromotor).
Forms of facial nerve palsy
Because the brain and nerves have a complex structure, damage at several locations can cause paralysis of the facial muscles.
Primary damage to the facial motor nucleus itself (nuclear paresis) is rare.
Central palsy
If the connection between the motor cortex and the motor nuclei in the brainstem (specifically in the pons) is damaged, this is called a central or supranuclear palsy. In such cases there are usually additional signs of central damage, for example weakness of the arms or legs. Central damage causes contralateral weakness of the mimic muscles, so a central lesion in the left brain presents as paralysis of the right side of the face. In central forms it is often still possible to wrinkle the forehead and to partially close the eyelid, because the upper facial muscles receive two-thirds of their innervation from the contralateral facial motor nucleus and one-third from the ipsilateral nucleus (Hacke 2016). Thus the muscles are weaker but can still move.
Peripheral palsy
The nerve is most commonly injured distal to the brainstem nuclei (infranuclear form). This is peripheral facial nerve palsy.
Symptoms of peripheral facial nerve palsy always occur on the same side as the lesion (ipsilateral). Usually the forehead and eyelid muscles are also affected. In addition, non-motor fibers may be involved, leading to taste disturbance and/or dysfunction of the salivary and lacrimal glands.
Causes of facial palsy
Inflammation
Inflammation can cause facial nerve palsy—then it is called facial neuritis. Here peripheral nerve disease is caused by viruses or bacteria. Common pathogens are neurotropic viruses, herpes viruses and bacteria.
Central (cerebral) damage
Cerebral dysfunction can lead to facial muscle paralysis and may have multiple causes: stroke (cerebral hemorrhage, infarction), multiple sclerosis, tumors, etc.
Peripheral damage
Paralysis resulting from peripheral damage—i.e., injury to the facial nerve (nervus facialis) itself—can have various causes.
- Idiopathic—of unknown cause. This accounts for 60–75% of cases (Finkensieper et al. 2012). Various other causes account for the remaining 25–40%.
- Traumatic. Temporal bone fractures can injure the facial nerve.
- Tumors. A tumor may encase, compress or displace the nerve. Various tumors can involve the nerve: parotid gland tumors, facial nerve schwannoma, acoustic neuroma, cerebellar tumors, tumor-related meningitis, etc.
- Iatrogenic (caused by medical intervention). Facial nerve injury can be a possible complication of surgical removal of the parotid gland or the infraorbital gland.
- As part of the following syndromes:
Guillain–Barré syndrome (acute inflammatory polyradiculoneuropathy), especially the Miller–Fisher variant (a form of GBS)
Carey Fineman–Ziter syndrome (congenital brain disorder)
Möbius syndrome (congenital developmental syndrome)
Melkersson–Rosenthal syndrome (inflammatory arterial disorder)
Heerfordt syndrome (inflammation of the parotid and lacrimal glands) - Facial nerve palsy can occur in metabolic diseases such as diabetes mellitus (especially when hypertension is also present).
- It can also occur during pregnancy (particularly in the last trimester) (Heckmann et al. 2017).
Depending on the cause, facial nerve palsy may have more specific names:
- Bell's palsy: idiopathic (of unknown origin) facial nerve palsy
- Ramsay Hunt syndrome: associated with zoster oticus infection
- Mona Lisa syndrome: palsy occurring during pregnancy
Symptoms of facial nerve palsy
Because the peripheral nerve is usually affected on one side, symptoms are typically unilateral—the facial nerve palsy affects only one half of the face. Bilateral facial palsy is rare and may occur, for example, in patients with borreliosis.
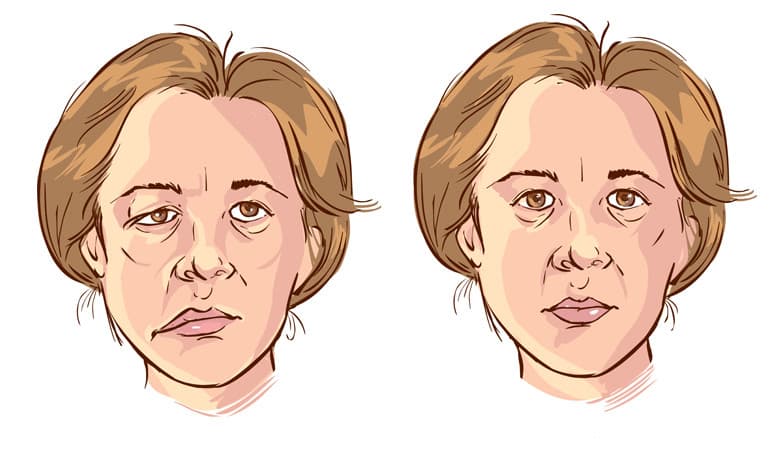
The main sign of facial nerve damage is paralysis of the mimic muscles:
- Drooping corner of the mouth
- Drooping eyelid
- Inability to wrinkle the forehead
- Paralysis of the orbicularis oculi often makes eyelid closure impossible. There is a risk of eye drying that must be treated symptomatically.
Beyond the muscles, facial nerve damage can affect other functions of the nerve:
- Reduced tear production
- Sound sensitivity (hyperacusis due to stapedius muscle dysfunction)
- Reduced saliva production
- Impaired taste (anterior two thirds of the tongue)
- Pain, numbness or tingling on one side of the face are not caused by the facial nerve damage itself, but may be observed in conditions involving other nerves (e.g., the trigeminal nerve).
Muscles on the healthy side "pull" the damaged side, making the face asymmetric. You cannot move the muscles on the affected side, resulting in an expressionless, mask-like appearance.
Prognosis
Idiopathic facial nerve palsy has a relatively good prognosis. In about 70% of cases the palsy resolves on its own within days or weeks, less commonly within months.
Only about 30% of affected patients develop a permanent motor deficit.
Synkinesias develop in about 16%—for example, involuntary simultaneous movement of the eye when closing the mouth (Peitersen 2002).
A first-time unilateral facial palsy also has a good prognosis, especially if patients are "young" (<60 years) and the nerve is only partially damaged (neurapraxia).
If the nerve is severely damaged or completely transected (axonotmesis), such as in a severe temporal bone fracture, complete recovery is unlikely. If full recovery does not occur, long-term facial asymmetry or synkinesis may develop.
Paralysis of the muscles around the mouth is not only psychologically distressing but also restricts daily functions. Flaccid muscles can cause drooling during drinking (saliva or liquids leak from the corner of the mouth), or food may remain on the cheek. Reduced muscle strength can affect speech; imprecise articulation makes understanding more difficult (dysarthria/speech disorder).
Symptomatic therapy and rehabilitation are particularly important for patients with severe injuries, permanent deficits, or difficulties with eating or speaking.
Treatment of facial nerve palsy
Sudden facial muscle paralysis—whether peripheral or central in origin—should always be treated as an emergency. Seek medical attention immediately.
If the cause is identifiable, treatment focuses on the underlying disease.
If the cause is unknown, standard drug therapy usually consists of steroids and/or antiviral medication.
Symptomatic treatment may also be necessary. If the eyelid cannot close, artificial tears, eye ointment and/or protective eye dressing are used to prevent corneal drying.
In severe, persistent pareses, microsurgical techniques may be used for facial nerve reconstruction, e.g., using the healthy nerve from the opposite side (cross-facial nerve grafting) or connecting the facial nerve with other nerves (hypoglossal–facial anastomosis). Forehead muscle transfer is another option. As research advances, surgical options continue to grow.
Facial paralysis can be shocking, but in the early phase focus on rest and treating the trigger. Adequate hydration and rest are important. Avoid exertion.
Several physiotherapy methods should be used in treatment
Electrotherapy
I already mentioned that some cases of palsy resolve spontaneously. The problem is that you cannot predict who will be lucky and recover within 1–2 months. Therefore treatment must be started as soon as possible.
Electrotherapy can be started early—3–4 days after the onset of paralysis. Most often it must be continued persistently for months, sometimes up to a year. Nerve fiber regeneration is very slow—typically 0.1–0.2 mm per day, and at best about 1 mm per day. The facial nerve can be 15–20 cm long, so you can see that even in the best case 150–200 days is the shortest possible time for regeneration.
You must perform electrical treatment 2–3 times daily because a denervated muscle (a muscle that has lost its motor nerve) atrophies quickly without motor impulses. Ultimately the muscle becomes irreversibly damaged, connective tissue proliferates and the condition cannot be restored.
Electrotherapy helps maintain muscle viability until regenerating nerve fibers reach the muscles again. If the muscle has been destroyed, symptoms will not improve even if the nerve regenerates. If viable muscle remains, muscle function can return.
Central palsy - ETS
In central palsy functional electrical stimulation (EMG-triggered electrostimulation), biofeedback, or a combination of both is used. Exercises target one or more muscles (1- or 2-channel) to restore function or to prevent involuntary movements. See my article on ETS—biofeedback-triggered stimulation.
Devices suitable for central palsy treatment include the Premium 400 multifunctional electrotherapy device and the DuoBravo N - ETS - biofeedback-triggered stimulation device.
Click the links for detailed information.
Peripheral paresis - denervated
In peripheral paresis the focus is on special currents (low frequency with long pulse duration). The more significant the nerve injury—especially after surgery—the more emphasis is on electrotherapy to protect muscles from atrophy and connective tissue changes.
The misconception that stimulation impedes reinnervation has been refuted by recent studies (Carraro 2018). In fact, low-frequency electrical stimulation has been shown to promote reinnervation (restoration of the muscle–nerve connection) (Gordon et al. 2016).
As recovery progresses and muscles become active again, synkinesis (e.g., involuntary eye movement when closing the mouth) often appears. Biofeedback therapy can help prevent these involuntary movements (Pourmomeny et al. 2014).
This is even more effective than mirror therapy alone (Dalla Toffola et al. 2012), although combining mirror therapy with biofeedback is certainly beneficial (Cardoso et al. 2008).
In general, good results are achieved when motor functions are strengthened by stimulation (Bernd et al. 2018), as is done in biofeedback therapy. Biofeedback can also be used in home therapy (Volk et al. 2014).
For peripheral palsy the so-called denervated treatment—called selective current therapy in domestic jargon—is appropriate. "Denervated" means a muscle that has lost its motor nerve.
I will mention two devices. The first is the German PeroBravo device, the second is the Italian Globus Genesy device family.
PeroBravo is a single-channel device specialized for treating peripheral palsy. Genesy models are 4-channel multifunctional electrotherapy devices; peripheral palsy treatment is only one of their functions, and they can help treat hundreds of other conditions as well.
PeroBravo offers an impressive arsenal of settings for treating peripheral palsy. These many options are best utilized by practitioners with extensive electrotherapy experience. Lay users can only make use of basic settings.
Genesy devices do not offer as many specialized denervated-program settings as the PeroBravo. Nevertheless, their basic programs are often excellent for most cases, and their extra functions and 4 channels make them a good choice, especially when other musculoskeletal problems exist.
Denervated treatment
When your face becomes paralyzed you will typically receive a few electrotherapy sessions at specialist clinics—usually 5–10 days. This outpatient treatment is certainly not enough, because even in the most favorable cases facial nerve palsy requires 3–4 months until symptoms subside. Most often 6–8 months are needed.
The ideal number of daily sessions is not one but 3–4. This cannot be accomplished at the clinic. It must be done at home. Obtain a stimulator device for this purpose.
Facial palsy is most commonly peripheral, where the facial muscles are denervated (they lose their motor nerve).
Denervated peripheral muscles cannot be stimulated by just any stimulator. You need a device capable of delivering slow-rise, long pulses (min. 200–400 ms, i.e., nearly half a second)—a device that provides denervated treatment.
A device bought at a discount supermarket is certainly not suitable for treating the facial nerve and facial muscles.
PeroBravo stimulator and denervated treatment
The PeroBravo device is produced by the German Berlin company MTR Plus. In Germany it is prescribed for peripheral palsy. At present it is not reimbursed here, so you must obtain it yourself.
PeroBravo was designed for treating peripheral paresis. Its programs 1–10 "follow" the course of paralysis.
Program 1 is intended for the most severe, complete nerve damage; as the program number increases it is optimized for less damaged nerve conditions.
Accordingly, in complete nerve injury start with Program 1 and advance to Program 2, then Program 3, and so on every few weeks as improvement occurs—until the nerve recovers and it can be stimulated well even with Program 10 (the latter program is for a healthy muscle–nerve connection).
Not every peripheral paresis is a complete nerve injury!
Therefore the appropriate starting program varies by case. In partial nerve lesions Program 1 may produce an unnecessarily long pulse that is uncomfortable and unneeded for the nerve. In such cases a higher-numbered program may be more appropriate.
If you are a physiotherapist you can perform intensity/duration curve determination. PRG 12 provides an automated diagnostic program for this. A professional can precisely determine the optimal treatment parameters for individual patients.
Usually your treating physician or physiotherapist should tell you which program is required. In my experience few doctors here will guide you in this regard.
If you have not received specific instructions, follow this strategy:
- Start with Program 07.
If you feel a subtle muscle twitch, continue this program.
If you do not feel muscle contraction, switch to Program 06. - If you still feel no twitch with 06, go to 05. Continue this way down to 01 if necessary. The latter is needed only in the most severe cases with complete nerve damage. The less severe the lesion, the closer you will be to 07.
- Continue with the program where you clearly feel muscle contraction.
Genesy 600, 1500 and 3000 devices
The Genesy devices are manufactured in Europe by the Italian company Globus, a producer of high-quality devices.
Genesy devices are multifunctional electrotherapy units suitable for treating hundreds of conditions.
Treating peripheral palsy is only one of their functions. Suitable models include Genesy 600, Genesy 1500 and Genesy 3000.
Although Genesy devices offer fewer denervated-specific settings than PeroBravo, their treatment capabilities and effects can be comparable.
Genesy 600 has one program each for severe, moderate and mild nerve damage, while Genesy 1500 and 3000 have three programs each. The latter allow the therapist to create a custom denervated program tailored to the individual patient's needs.
Treatment programs can be found under Program List / Medical Treatments / Denervated program group.
- Triangular pulse is used for severe nerve damage.
- Trapezoid pulse is used for partial damage.
- Square pulse is used for mild damage.
Stimulation treatment of the paralysed facial muscles
The facial nerve has three main branches that supply many facial muscles. In the illustration below you can see a dozen muscles on the forehead, around the eye, around the mouth, on the jaw and on the cheek.
Which branch and which specific muscle is most affected varies from case to case. Some patients have problems in all three branches, others only in a smaller area.
Treatment should be performed according to where your symptoms are. Each muscle should be treated individually because the degree of damage can differ and a different program may be required for each muscle.
Use small (approx. 25 mm), round electrodes for treatment. Suitable are PALS Round 25mm or ValueTrode Round 32mm.
In the illustration you see multiple points. Connect the negative pole of the cable (usually marked by a black connector) to the electrode placed near the ear. This electrode remains in place. Place the other, positive electrode (red connector) on the first point (for example, the forehead).
Perform the treatment. When finished, move the positive electrode to the next point (corner of the eye), keeping the negative at the ear. Perform the treatment there as well. Continue sequentially through all required points.
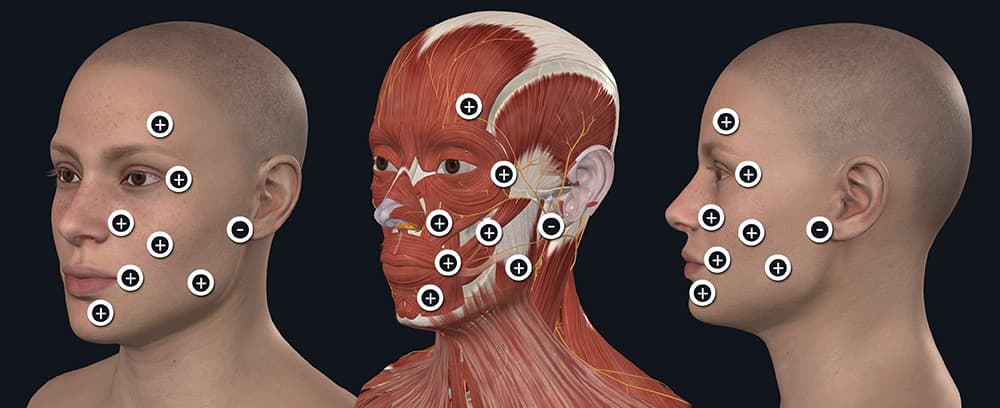
When treating facial nerve palsy (Bell's palsy) many points along the facial nerve must be treated. Use small (approx. 25 mm), round electrodes. Always place the negative pole near the ear. The positive pole position must be changed. Start on the forehead, and when the treatment time ends, move the electrode and treat the next point. It is not necessary to treat every illustrated point in every case—ask your physiotherapist for guidance!
Adjust current intensity carefully. Increase until you feel muscle contraction. Then gradually raise the intensity from session to session until muscle contraction is definite but not painful.
Facial muscles are very small, so a muscle twitch can be detected at very low intensity—2–3 mA.
If you have sensory loss, be cautious because you may not feel the impulses and could raise the intensity too high. Excessive current intensity can cause skin damage similar to burns.
How to make it more effective!?
Stimulation treatment is more effective when combined with mimetic exercises in front of a mirror!
When you feel the device impulse and muscle contraction, watch your face and voluntarily "help" the movement. Visual input from your sight also sends stimulatory signals toward the damaged facial nerve.
This combined treatment significantly enhances regenerative activity and thus improves the efficiency and speed of recovery!
Soft laser treatment
Another important method for treating facial nerve palsy is soft laser therapy. I consider class 3 laser devices appropriate for this, for example the Personal Laser L400 and the Energy Laser L500 Pro. Read my article about soft lasers: Basics of soft laser devices and treatments. From that you can learn that class 3 lasers are the most powerful lasers that can be issued for home use. Treatment is fast and effective.
Importance of immediate soft laser treatment
The main reason for facial nerve palsy is that the nerve fiber swells (becomes edematous) and thus becomes "trapped" in the bony canal through which it passes.
The nerve fiber is damaged because the swelling presses it against the bone, impairing its blood supply and function. If we reduce the edema around the nerve fiber, we can minimize nerve damage.
Soft laser treatment should be started as quickly as possible after onset of facial nerve palsy.
Soft laser therapy stimulates microcirculation, and improved blood flow reduces edema.
Edema reduction is a short-term effect of laser therapy.
Importance of prolonged soft laser treatment
The brain and nerves are very sensitive. In most cases many hours pass between the onset of palsy and hospital admission and completion of examinations.
Consequently, the nerve fiber is already somewhat damaged by the time the first treatments begin.
Facial nerve palsy (nerve damage) is among the slowest-to-heal conditions. Even in ideal cases, months of treatment are required to reduce symptoms.
Although some cases of facial nerve palsy may heal spontaneously, it is impossible to predict who will be fortunate.
Therefore physiotherapy, electrotherapy and soft laser treatments must be applied for a long period (usually a minimum of 3–6 months).
Soft laser treatment supports nerve regeneration and thus accelerates the healing process.
Recommended professional literature for specialists: Aghamohamdi D, Fakhari S, Farhoudi M, Farzin H. The Efficacy of Low-Level Laser Therapy in the Treatment of Bell's Palsy in Diabetic Patients. J Lasers Med Sci. 2020 Summer;11(3):310-315. doi: 10.34172/jlms.2020.52. Epub 2020 Jun 21. PMID: 32802293; PMCID: PMC7369545.
Soft laser treatment of facial nerve palsy
The facial nerve has three main branches that supply the facial muscles. Not all three branches are necessarily equally affected in your case.
In the illustration below you see many potential treatment points.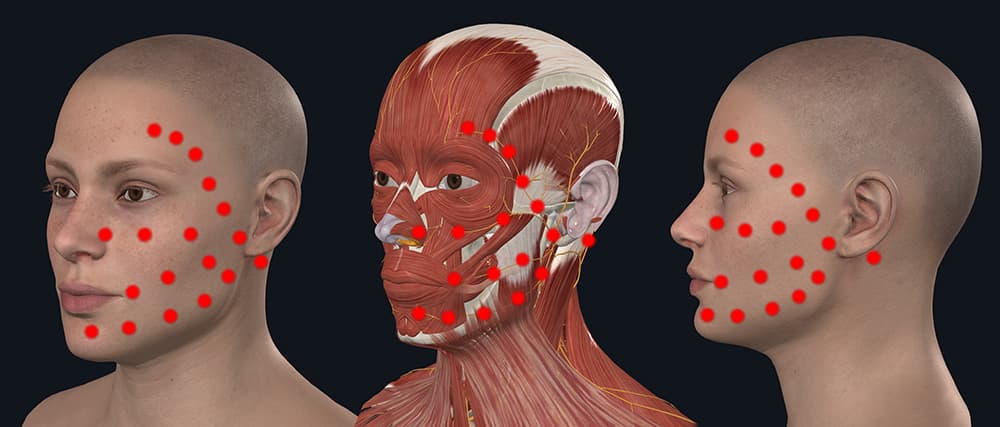
If you cannot close your eyelid but the other branches are preserved, it may be sufficient to treat only the upper two lines toward the ear.
If you cannot wrinkle your forehead, cannot close your eye, and your mouth corner droops so you cannot "pucker," then all points must be treated.
Always start treatment at the point behind the ear. Never skip this point.
Then treat from the midline along the course of the nerve toward the ear.
At each point hold the device for a specified time. Required time depends on device power. Preferably hold the device perpendicular to the skin and let it touch your skin.
Treatment with the Personal-Laser L400
The Personal-Laser L400 is the world's smallest class 3 soft laser. It is only slightly thicker and longer than a man's thumb. Its battery provides about 2 hours of treatment on a single charge.
The laser beam area is 1 cm2. The small spot diameter makes it excellent for local treatment of facial nerve palsy.
The laser wavelength is 808 nm (infrared), invisible to the eye. The device's red light is not the laser itself; it is only an aiming light and operation indicator.
The laser emits 400 mW continuous power. This means it emits 4 Joules every 10 seconds and signals this with a beep.
Unless your treating physician directs otherwise, follow this general treatment plan for the Personal-Laser L400.
| 1st week | From week 2 until symptom resolution | |
| Point behind the ear | 3 beeps (12 Joule) | 2 beeps (8 J) |
| Other points along the facial nerve | 2 beeps (8 J) | 1 beep (4 J) |
Treatment with the Energy-Laser L500 Pro
The Energy-Laser L500 Pro is a class 3 soft laser. Its battery provides about 1.5 hours of treatment on a single charge.
The laser beam area is 1 cm2. The small spot diameter makes it excellent for local treatment of facial nerve palsy.
The laser wavelength is 808 nm (infrared), invisible to the eye. The device's red light is not the laser itself; it is only an aiming light and operation indicator.
The laser emits 500 mW continuous power. This means it emits 5 Joules every 10 seconds and signals this with a beep.
Unless your treating physician directs otherwise, follow this general treatment plan for the Energy-Laser L500 Pro.
| 1st week | From week 2 until symptom resolution | |
| Point behind the ear | 2 beeps (10 Joule) | 1 beep (5 J) |
| Other points along the facial nerve | 1 beep (5 J) | 1 beep (5 J) |
What outcome can be expected?
Patients with Bell's palsy often ask me: "I developed Bell's palsy a year ago. I had exercises, soft laser treatments, acupuncture, but unfortunately I don't see much improvement. The left corner of my mouth 'hangs' as if I came from the dentist. What are my prospects?"
Well... this is in the realm of "fortune-telling."
It is impossible to predict the future over the Internet or even at a personal consultation. The outcome of medical treatment depends on countless factors. For example:
- Was treatment started in time? Months after onset there is little that can be done. Treatment should begin on the day of onset (medication, soft laser, electrotherapy).
- Are treatments performed long enough? Most patients believe that the clinic's 5–10 physiotherapy sessions, the same number of soft laser sessions and electrotherapy sessions are sufficient.
They are NOT!
Therapy must be persistent and improvement is generally expected after 3–6 months. Many patients require treatment for over a year. - How are they treated? Treatment with inappropriate devices, for an insufficient duration, or at incorrect treatment points is meaningless and ineffective. It is therefore very important what and how you treat.
Bell's palsy heals spontaneously without treatment in a minority of cases. The problem is you cannot know in advance who will be that lucky person. Those who are not in the fortunate group will not improve without treatment.
Therefore daily, persistent treatment is necessary—sometimes for up to 1.5–2 years. If there is no change after such a period... well, such cases do occur. In some cases persistent treatment yields no result, fortunately a smaller group.
If you carry out treatments with the appropriate frequency, that is:
- facial exercises 4–5 times daily for 10–15 minutes each,
- electrotherapy at least once daily, ideally multiple times daily,
- soft laser every day or every other day,
then you can be optimistic that improvement will occur (though even then 100% recovery is not guaranteed).