

 Microcurrent therapy at home: what you need to know before you start?
Microcurrent therapy at home: what you need to know before you start?
I presented the theoretical background of the method in the microcurrent and its effects main article; joint-specific clinical evidence is discussed in the microcurrent therapy and joint inflammations article. This piece focuses on the practical aspects.
 Key idea
Key idea
The success of microcurrent treatment depends on three things: (1) the correct indication (according to recent clinical evidence, acute knee pain [1] and postoperative rotator cuff pain [2] are the most studied areas), (2) correct electrode placement (around the painful area, not on the single most painful spot), and (3) patience – effects typically become noticeable after 2–4 weeks of regular treatment [3]. The method is an adjunct modality: it does not replace medical diagnosis, medication, or an exercise program.
 When is it worth using microcurrent at home?
When is it worth using microcurrent at home?
Recent (2020+) clinical evidence shows measurable benefit in the following areas when used as an adjunct to standard care. In each case it should be used as a complementary therapy alongside medical diagnosis and management:
A double-blind trial of 52 patients [1] found a statistically significant improvement in acute knee pain by week 3. A systematic review [3] assigned a high level of evidence (GRADE) to this indication. In osteoarthritis-related complaints microcurrent may contribute to pain relief, but it does not regenerate cartilage – basic care (exercise program, weight control, physiotherapy, NSAIDs) remains the cornerstone.
A 28-patient RCT [2] showed significantly greater improvements in pain, shoulder function, and grip strength in the microcurrent group after rotator cuff repair. Important context: a larger 2025 trial [4-like NMES comparison] found NMES to be more effective – microcurrent is therefore a possible, but not necessarily the superior, option in postoperative rehab. Discuss with your treating physician which method they recommend.
A 2025 double-blind crossover trial of 71 patients [6] (largely patients with thoracic pain) found kHz-range microcurrent reduced average pain by 2.2 NRS points. Important: clarify the diagnosis behind back pain (disc herniation, spinal degeneration, muscle-origin pain) medically before self-treating at home.
An 18-subject, 8-week study [4] showed that post-workout microcurrent application (3 hours daily) reduced the sensation of DOMS at 24 and 48 hours. Important: the study did not improve aerobic performance – microcurrent does not guarantee increased training efficiency, but it may aid recovery.
A 2022 meta-analysis [7] (8 RCTs, n=337) found that microcurrent plus standard wound care reduced wound area by 8.3 cm² and shortened healing time by 7 days versus standard care alone. Important: wound healing management is a specialist task; home microcurrent treatment is only recommended as an adjunct under specialist supervision. Details: leg ulcer with electrostimulation for healing.
 Preparations: what do you need before treatment?
Preparations: what do you need before treatment?
Due to microcurrent's low intensity its safety profile is favorable, but treatment success depends on proper preparation. You should prepare in three areas:
A multifunction device with microcurrent capability requires three accessories:
- The device (Premium 400, Globus Genesy 1500/3000, or TensCare UniPro) charged and ready
- Connection cables (use factory-supplied cables – microcurrent channels often have specially marked shielded cables)
- Self-adhesive electrodes (CE-marked; typically 50×50 mm square or 50×100 mm rectangle)

Store electrodes in a cool, dry place and replace them according to the manufacturer's lifespan (typically 15–30 uses). Worn, dry, or infected electrodes increase the risk of skin irritation and can reduce treatment effectiveness.
Electrode-to-skin contact quality directly affects treatment effectiveness:
- Cleaning: wash the treatment area with lukewarm soapy water and dry thoroughly.
- Hair removal: if the area is densely hairy, shave beforehand (24 hours before treatment to allow irritation to settle).
- Avoid creams and cosmetics: body lotion, oil, deodorant can insulate – do not apply them before electrode placement.
- Check for skin lesions: do not place electrodes over a fresh wound, extensive eczema, or infection.
Before each session it is worth running through:
- Contraindication list (see below): pacemaker, pregnancy, malignancy, acute fever, DVT, etc.
- Cable and electrode condition: do not use damaged cables or delaminated self-adhesive electrodes.
- Device charge: a device running out of battery during treatment is undesirable.
- Confirmed diagnosis: for new, worsening, or unexplained complaints seek medical consultation before self-treatment.
Electrode placement: where to put the self-adhesive pads?
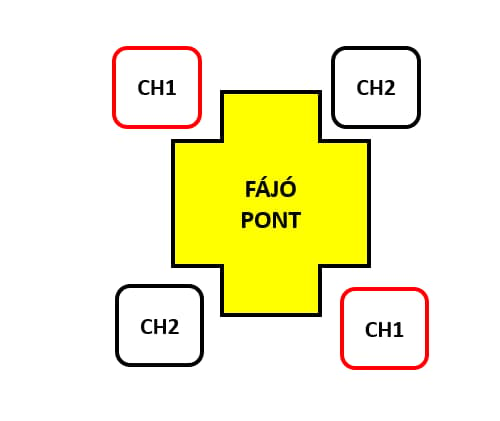
One of the most common errors in microcurrent therapy is incorrect electrode positioning. The basic principle: current flows between the two electrodes, so place them so that the current "passes through" the painful area. Do not place an electrode on the single most painful point – position the electrode pair AROUND the painful area.
| Rule | Detail |
|---|---|
| Number of electrodes per channel | 2 pcs (negative + positive) |
| Position | on BOTH SIDES of the painful area, not on the focus |
| Minimum distance between electrodes | 2–3 cm (below this current concentration may occur) |
| Maximum distance | 20 cm (above this current density may be too low) |
| Skin contact | adhere over the full surface – no air insulation |
| Surgical scar, screw, plate | do not place electrodes over these – consult the treating physician |
| Pacemaker, ICD | avoid near the chest – only with cardiologist approval |
Indication-specific placements:
- Knee joint: 2 electrodes above and below the patella (on the medial or lateral side) so the current covers the whole knee joint.
- Shoulder joint: one electrode on the upper deltoid and one on the lower part (over the rotator cuff area).
- Back pain (lumbar): 2 electrodes on both sides of the painful vertebral segment (paravertebral), about 5 cm from the midline of the spine.
- Elbow (epicondylitis – "tennis elbow"): one electrode on the upper forearm and one on the middle forearm – surrounding the painful bone attachment point.
- Achilles tendon / plantar fascia inflammation: one electrode on the lower third of the calf, and one on the heel or the arch of the foot.
Typical protocol parameters
Microcurrent devices come with built-in programs – factory settings are usually a good starting point. The table below summarizes ranges used in recent clinical studies [1][2][6][7] so you understand what the device sets:
| Parameter | Range | Note |
|---|---|---|
| Current intensity | 50–600 µA | Sub-sensory – typically not felt. ≥1000 µA (1 mA) is no longer microcurrent! |
| Frequency | 0.3–500 Hz | Depends on device program; low-to-mid Hz most common |
| Treatment duration | 30–60 minutes | Knee study [1]: 3 hours daily (home, longer protocol) |
| Frequency | 1–3 times daily | Shoulder study [2]: 3 times weekly for 4 weeks |
| Program period | 4–8 weeks | Effects begin to appear after 2–4 weeks |
| Wound-healing protocol [7] | 10 hours daily, 25 days | ONLY under specialist supervision |
Key idea – intensity setting
For microcurrent you do not need to adjust the intensity as you would with TENS or EMS – factory programs provide a µA value that typically remains constant during treatment. Do not modify factory settings "to be sure of the effect": above 600 µA the modality is no longer microcurrent but mini‑TENS, which changes the nature of the treatment.
Starting the treatment – step by step
- Turn on the device. Check the battery level.
- Connect the cable to the device. The microcurrent channel is often marked (e.g., shielded grey cable in Globus systems).
- Connect the electrodes to the cable end (snap connector).
- Place the electrodes on the skin according to the instructions above (on both sides of the painful area, minimum 2–3 cm apart).
- Select the program from the device menu (MENS/Microcurrent category, subprogram appropriate to the indication).

- Start the treatment. Microcurrent programs use factory-set intensities; manual adjustment is usually unnecessary. The channel 1 intensity button indicates the treatment is running.

- During treatment sit or lie down comfortably – no movement is required (unlike EMS training).
- At the end of the session the device stops automatically. Remove the electrodes (do not yank the cable).
- Electrode storage: put the pads back on the protective film and store in a cool, dry place.
 Common mistakes and how to avoid them
Common mistakes and how to avoid them
- "I feel nothing, it surely doesn't work." – Microcurrent is sub-sensory; you typically do not feel it during the session. This is normal. Effects usually begin to appear after 2–4 weeks.
- Electrode in the wrong place. An electrode placed on the single most painful spot is not optimal – place the pair AROUND the painful area so the current crosses it.
- Cream or lotion on the skin. Their insulating effect reduces electrode contact. Always place electrodes on clean, dry skin.
- Too dense hair. Also reduces contact. Shaved areas provide better effectiveness.
- Stopping too early. Clinical trials [1][2] reported meaningful improvement after 3–4 weeks. Quitting after 1–2 sessions because you "didn't feel an effect" is premature.
- Searching for higher intensity. Above 600 µA the treatment is no longer microcurrent – you may be needlessly increasing intensity.
- Replacement mentality. Microcurrent DOES NOT replace medication or an exercise program – it is additive, not an alternative.
- Near surgical materials. Do not place electrodes over fresh surgical wounds, screws, plates, or staples – consult your treating physician.
How long until you can expect change?
Recent clinical study timelines show the following:
- 24–48 hours: in sports recovery [4] the sensation of DOMS may be reduced after training.
- 2–3 weeks: in acute knee pain [1] a statistically significant pain reduction was seen by week 3 compared to control.
- 4 weeks: in rotator cuff postoperative rehab [2] measurable functional improvement was observed after a 4‑week program (3 sessions weekly).
- 14–25 days: for hard-to-heal wounds (e.g., pressure ulcers) [7] improvements of 16–25% on the PUSH scale were seen during the treatment period – this is a specialist-supervised protocol.
- 2–4 weeks: for most chronic complaints this is the starting timeframe to observe meaningful change.
If you do not feel any change after 6–8 weeks of regular treatment, seek medical or physiotherapy consultation – the underlying diagnosis may require a different approach. Do not continue indiscriminately "hoping it will work" without review.
Home devices with microcurrent programs
In the Medimarket portfolio the following multifunction devices include factory MENS protocols:
- Premium 400 – 4 channels, factory MENS programs for joint support and wound healing.
- Globus Genesy 1500 – 2 channels, base package microcurrent + TENS + EMS for home multifunction use.
- Globus Genesy 3000 – 4 channels, expanded program selection for sport and rehab use.
- TensCare UniPro – compact 2‑channel device with simplified TENS, EMS and MENS programs.
For electrodes: self-adhesive TENS/EMS/MENS electrodes (the same pads are suitable for microcurrent).
 When is microcurrent treatment NOT recommended?
When is microcurrent treatment NOT recommended?
Details of general electrotherapy contraindications are discussed in the electrical treatment contraindications and electrical treatment and implants articles.
- Pacemaker, ICD, implanted neurostimulator – only with cardiologist/arrhythmologist approval.
- Active malignant tumor in the treatment area – regenerative effects could pose a risk.
- Pregnancy – avoid for maternal and fetal safety reasons.
- Acute joint inflammation with fever or unexplained origin – medical evaluation first.
- Active venous thrombosis (DVT) in the treatment area – risk of embolization.
- Fresh skin wound, extensive eczema, skin infection at the electrode site.
- Carotid sinus / anterior neck region – do not place electrodes near the carotid artery.
- Placement over the chest/heart – avoid even without a pacemaker (risk of rhythm disturbance).
- Skull, temples – electrical treatment should not be applied to the head with a home device.
- Over the thyroid – avoid.
- Epilepsy with poor medication control – individual assessment required.
- Severe sensory deficit in the treatment area – makes safe self-treatment difficult.
For new, worsening, or unexplained complaints always seek medical consultation before starting self-administered microcurrent treatment.
Frequently asked questions about the practical use of microcurrent therapy
Clinical studies used varied protocols: 1 hour daily [similar to study 2], 3 hours daily [1], or for special wound-healing protocols 10 hours daily [7]. For home use factory programs typically recommend 30–60 minute sessions, 1–3 times per day. Exact settings depend on the indication and device type – follow the manufacturer's instructions.
The microcurrent range (50–600 µA) is sub-sensory for most users, i.e., below perception threshold. This is normal and does not indicate ineffectiveness – it is a designed property of the method. If you increase intensity above 600 µA you will no longer have microcurrent but a mini‑TENS sensation, which changes the treatment's character.
Clinical trials indicate meaningful effects after 2–4 weeks of regular treatment. In acute knee pain [1] improvement was statistically significant at week 3; in rotator cuff studies [2] functional gains were measured after a 4‑week program. In sports recovery [4] DOMS may decrease within 24–48 hours. Patience is required – microcurrent is not an immediate fix.
Yes, but in separate sessions. The Premium 400, Genesy 1500/3000 and TensCare UniPro all offer multiple program families (TENS, EMS, MENS), but they cannot be combined simultaneously on the same channel – each works with different parameters and goals. You can apply different treatment types on the same day (e.g., EMS training in the morning, MENS recovery in the evening).
CE-marked self-adhesive electrodes are typically designed for 15–30 uses (depending on manufacturer specifications). Replace electrodes if they are worn, dry, detach from the skin, or the adhesive no longer sticks properly. Proper storage (on the original protective film, in a cool, dry place) can extend their lifespan.
No, it does not replace them. Recent reviews [3][5] position microcurrent as an adjunct modality. Decisions about stopping, reducing, or changing medication are exclusively the treating physician's responsibility. NSAID risks (gastrointestinal, renal, cardiovascular) are real, and their management cannot be solved solely by microcurrent devices – appropriate medication choice is a medical task.
 Summary – fundamentals of successful home microcurrent treatment
Summary – fundamentals of successful home microcurrent treatment
What every home user should know
- 50–600 µA range, typically not felt – this is normal and not a malfunction.
- Electrode placement: on BOTH SIDES of the painful area, minimum 2–3 cm apart.
- Treatment duration: 30–60 minutes, 1–3 times daily, for 4–8 weeks.
- Effect: starts to become noticeable after 2–4 weeks – patience is required.
- Proven indications (2020+ evidence): acute knee pain [1], rotator cuff rehab [2], chronic back pain [6], sport recovery [4], hard-to-heal wounds (under specialist supervision) [7].
- Skin preparation: clean, dry skin without creams or cosmetics.
- Avoid replacement mentality: microcurrent is an adjunct modality, not an alternative to medication or exercise programs.
- Contraindications (pacemaker, pregnancy, malignancy, acute fever, DVT) must be strictly observed.
- If there is no change after 6–8 weeks: medical or physiotherapy consultation is necessary.
Scientific sources (2020+)
The references [1]–[7] cited in the article refer to the following studies (list order = ol list):
- Lawson D, Lee KH, Kang HB, Yang N, Llewellyn T, Takamatsu S. Efficacy of microcurrent therapy for treatment of acute knee pain: A randomized double-blinded controlled clinical trial. Clinical Rehabilitation. 2021;35(3):390-398. PMID: 33095658.
- Yi D, Lim H, Yim J. Effect of Microcurrent Stimulation on Pain, Shoulder Function, and Grip Strength in Early Post-Operative Phase after Rotator Cuff Repair. Medicina (Kaunas). 2021;57(5):491. PMID: 34067980.
- Iijima H, Takahashi M. Microcurrent Therapy as a Therapeutic Modality for Musculoskeletal Pain: A Systematic Review Accelerating the Translation From Clinical Trials to Patient Care. Archives of Rehabilitation Research and Clinical Translation. 2021;3(3):100145. PMID: 34589695.
- Naclerio F, Moreno-Perez D, Seijo M, Karsten B, Larrosa M, García-Merino JÁ, Thirkell J, Larumbe-Zabala E. Effects of adding post-workout microcurrent in males cross country athletes. European Journal of Sport Science. 2021;21(12):1708-1717. PMID: 33295832.
- Jonik S, Rothka AJ, Cherin N. Investigating the therapeutic efficacy of microcurrent therapy: a narrative review. Therapeutic Advances in Chronic Disease. 2025;16:20406223251361677. PMID: 40821620.
- Martuliak I, Chvála Ľ, Ferenčík M, Fabián V, Slovák M. Efficacy of Rebox Electrotherapy in Pain Management: A Randomized Double-Blind Sham-Controlled Crossover Trial. Pain and Therapy. 2025;14(5):1597-1610. PMID: 40900299.
- Avendaño-Coy J, López-Muñoz P, Serrano-Muñoz D, Comino-Suárez N, Avendaño-López C, Martin-Espinosa N. Electrical microcurrent stimulation therapy for wound healing: A meta-analysis of randomized clinical trials. Journal of Tissue Viability. 2022;31(2):268-277. PMID: 34903470.

This article is for general informational purposes and does not replace personal medical consultation. Microcurrent therapy (MENS) is an adjunct modality; it does not replace medication, exercise programs, or surgical care. Contraindications (pacemaker, malignancy, pregnancy, acute febrile condition, DVT) must be strictly observed. The devices shown are CE-marked medical devices; the referenced clinical trials used various devices and protocols. Individual results may vary. For new, worsening, or unexplained complaints consult your treating physician or physiotherapist.