

Muscle stimulation is an effective complement to pelvic floor muscle training. The Cochrane Institute's comprehensive 2022 review confirmed that PFMT complemented with electrostimulation can produce better results than exercises alone.1
 Key point
Key point
Consistency is the key to success. Electrostimulation treatment – like exercise – only works with regular application. Twenty to thirty minutes daily for a minimum of 8–12 weeks.
Why use a muscle stimulator?
Pelvic floor muscle training (Kegel exercises) is effective on its own, but about 30% of affected people cannot voluntarily contract these muscles correctly. An electrostimulator elicits muscle contraction with low‑intensity pulses – in a targeted and concentrated way.
| Method | Advantage | Expected result |
|---|---|---|
| Kegel exercises alone | Can be done anywhere, free | 2–4 months of regular exercise |
| Kegel + electrostimulation | Targeted, more intense, measurable | Noticeable improvement after 2–4 weeks |
| Kegel + ES + biofeedback | Objective feedback, lasting effect | 2–4 weeks + sustained maintenance |
 Important
Important
Medical evaluation is required before starting treatment to determine the type of incontinence. Stress, urge, mixed and fecal incontinence require different treatment protocols. Read about the types here →
 Treatment protocols – by type
Treatment protocols – by type
The type of incontinence matters! Choosing the correct program is the foundation of successful treatment. The following settings are commonly used (some devices may have different built‑in programs).
Goal: Increase the strength of the pelvic floor muscles and sphincter.
Frequency: 35–50 Hz (fast contractions)
Pulse: 200–300 µs pulse width, alternating cycle (work/rest: e.g. 5 sec / 10 sec)
Treatment time: 20–30 minutes/session
Frequency: First 2 weeks: every other day, then: daily
Duration: Minimum 8–12 weeks
Goal: Calm bladder overactivity and reduce involuntary contractions.
Frequency: 10–20 Hz (slow, soothing stimulation)
Pulse: ~200 µs pulse width, continuous or slow cycling
Treatment time: 20 minutes/session
Frequency: Daily or every other day
Duration: Minimum 8–12 weeks
Goal: Tension reduction + muscle training – in two phases.
Phase 1: Bladder‑calming program (10–20 Hz) – 10 minutes
Phase 2: Muscle training program (35–50 Hz) – 15–20 minutes
Frequency: Daily (most devices handle the two phases automatically)
Duration: Minimum 12 weeks
Goal: Increase the strength of the anal sphincter.
Frequency: 35–50 Hz
Pulse: 200–300 µs, alternating cycle
Electrode: Rectal probe (recommended) or upper‑thigh electrode
Treatment time: 20 minutes/session
Duration: Minimum 12–16 weeks (improvement is usually slower)
 Electrode and probe placement
Electrode and probe placement
Incontinence treatment can be performed with self‑adhesive surface electrodes attached to the skin or with an intracavitary probe (vaginal/rectal). Probe treatment is generally more effective because the pulses act directly on the pelvic floor muscles.
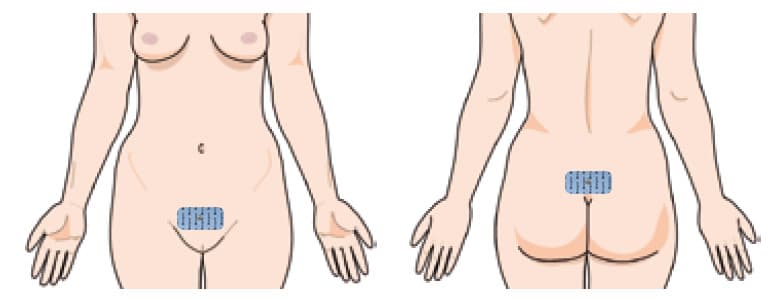
1. Transcutaneous stimulation: pubic mound – sacrum
Use two large surface (50×90 mm) self‑adhesive electrodes. Place one on the pubic mound (for men about 2–4 cm above the base of the penis), the other on the sacrum. The electrodes connect to the two ends of the same stimulation cable.
 Note
Note
This placement is widely recommended, but due to the large electrode distance it is less targeted. A more effective alternative can be the upper‑thigh placement (see below).
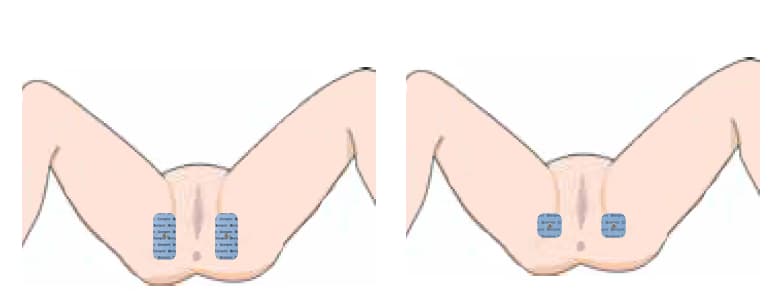
2. Transcutaneous stimulation: upper inner thighs
Place the electrodes bilaterally in the groin folds so that the vaginal or anal opening lies between them. Leave about a palm's width between the two electrodes. This method is more effective because the pulse passes directly through the pelvic floor.
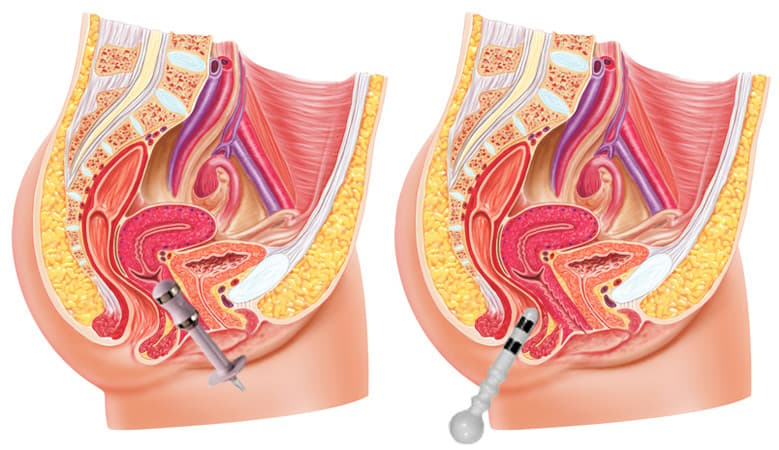
3. Intracavitary probe stimulation
The vaginal or rectal probe sits close to the pelvic floor muscles, making this the most targeted treatment method. Insert the vaginal probe about 3–5 cm deep as you would a tampon. Insert the rectal probe 2–3 cm deep up to the level of the internal sphincter.
Which to choose?
If there are no contraindications, the intracavitary probe is recommended – it provides more effective treatment. Use self‑adhesive electrodes if probe insertion causes discomfort or if local issues such as hemorrhoids or fissures are present.
 Treatment process – step by step
Treatment process – step by step
1. Find a calm, private place. A session lasts 20–30 minutes.
2. Do NOT switch on the device yet.
3. Connect the electrodes/probe to the cable, and the cable to the device.
4. Self‑adhesive electrode: pre‑gelled, do not wet. Probe: moisten with water or lubricating gel – this aids insertion and impulse transmission.
5. Get comfortable – sitting, semi‑reclined or lying down.
1. Switch on the device and select the program appropriate for your symptoms.
2. Slowly increase the intensity (plus button). At first you feel nothing, then a mild tingling, and finally distinct muscle contractions.
3. For probes the typical range is 10–30 mA. Do not exceed 30 mA.
4. If the sensation is unpleasant or painful, reduce the intensity by a few steps. The treatment should not be painful.
5. With probes, use small movements to find the position where you feel the strongest contraction.
6. The device usually stops automatically at the end of the program.
1. Turn off the device.
2. Self‑adhesive electrode: remove and stick back onto the plastic backing.
3. Probe: remove it by holding its rim (not the cable). Clean with lukewarm water.
4. Do not put it in boiling water and avoid corrosive cleaners. You may use disinfectant solution or wipes.
5. Dry and store in a clean, dry place.
Daily routine and schedule
Treatment effectiveness hinges on regularity. Here is the recommended schedule:
| Period | Frequency | What to expect? |
|---|---|---|
| Weeks 1–2 (introduction) | Every other day, 15–20 minutes | Getting used to it, "awakening" the muscles |
| Weeks 3–8 (intensive phase) | Daily, 20–30 minutes | Noticeable improvement, reduced leakage |
| Weeks 9–12 (stabilization) | Daily, 20–30 minutes | Significant improvement, quality‑of‑life change |
| After week 12 (maintenance) | 1–2 times per week | Preserve achieved result |
Morning or evening?
The time of day does not matter – do it when you can calmly devote 20–30 minutes. Many do it in the evening while relaxing, watching TV or reading. The point is consistency, not timing.
 Important
Important
If symptoms improve, do not stop treatment completely! Maintenance sessions (1–2 times weekly) are necessary to preserve results. If you stop, the muscles may gradually weaken.
Which device to use?
When selecting a device, the type of incontinence and the need for biofeedback are decisive:
| Device | Programs | For whom? |
|---|---|---|
| Kegel Toner | Stress incontinence | Mild symptoms, entry level |
| Perfect PFE Women | Stress + urge | Women with moderate symptoms |
| Perfect PFE for Men | Stress + urge (male) | Men, post‑prostate surgery |
| Biolito | Stress + urge + mixed | Both sexes, good value |
| Myolito | Incontinence + pain (TENS/EMS/FES) | Multifunctional needs |
| evoStim UG | Complex protocols | Severe incontinence |
| evoStim E | All types + EMG biofeedback | Measurable progress, complex cases |
| evoStim P | All types + pressure biofeedback | Complex cases, fecal incontinence |
Find the full range on the incontinence devices category page.
 When not to use it?
When not to use it?
- Cardiac pacemaker
- Pregnancy
- Active cancer in the treatment area
- Untreated epilepsy
- Acute inflammation or infection in the pelvic/rectal area
Do not use a probe in the presence of hemorrhoids, anal fissure, fistula or acute local inflammation. In such cases, self‑adhesive electrode treatment is the recommended alternative.
 Frequently asked questions
Frequently asked questions
No. You will feel a mild tingling and distinct muscle contractions. If you experience pain, reduce the intensity. The treatment should never be painful.
A probe is more effective because it works close to the pelvic floor muscles. Choose self‑adhesive electrodes if probe insertion is uncomfortable or if a local problem (hemorrhoids, fissure) exists.
Yes. Movement does not reduce effectiveness – you can stand up or walk. Many perform the session while reading or watching TV – the important thing is to be comfortable.
Try gradually increasing the intensity. With a probe, make small positional adjustments. If you still do not feel contractions, a device with biofeedback (e.g. evoStim E) can help you learn the correct technique.
A minimum of 8–12 weeks of intensive treatment is recommended. If symptoms improve, you can switch to maintenance (1–2 sessions per week). If you stop completely, the muscles may gradually weaken and symptoms can recur.
 Read more
Read more
Summary – Quick overview
Source
- Todhunter‑Brown A, Hazelton C, Campbell P, et al. (2022). Conservative interventions for treating urinary incontinence in women: an Overview of Cochrane systematic reviews. Cochrane Database Syst Rev. 9(9):CD012337. DOI: 10.1002/14651858.CD012337.pub2
